

Complete intracranial response to talimogene laherparepvec (T-Vec), pembrolizumab and whole brain radiotherapy in a patient with melanoma brain metastases refractory to dual checkpoint-inhibition
- PMID: 29622046
- PMCID: PMC5887256
- DOI: 10.1186/s40425-018-0338-6
Complete intracranial response to talimogene laherparepvec (T-Vec), pembrolizumab and whole brain radiotherapy in a patient with melanoma brain metastases refractory to dual checkpoint-inhibition
Abstract
Background: Immunotherapy, in particular checkpoint blockade, has changed the clinical landscape of metastatic melanoma. Nonetheless, the majority of patients will either be primary refractory or progress over follow up. Management of patients progressing on first-line immunotherapy remains challenging. Expanded treatment options with combination immunotherapy has demonstrated efficacy in patients previously unresponsive to single agent or alternative combination therapy.
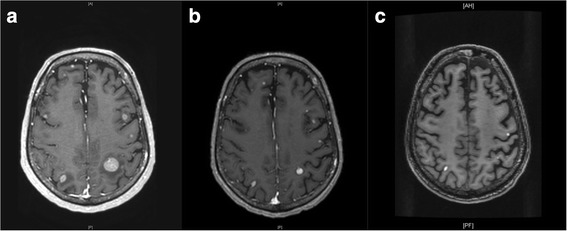
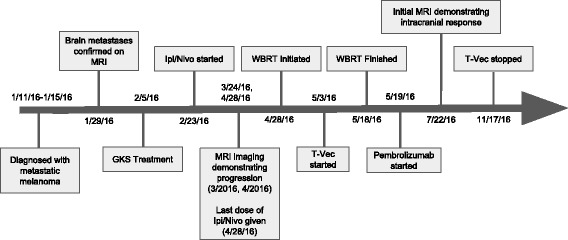
Case presentation: We describe the case of a patient with diffusely metastatic melanoma, including brain metastases, who, despite being treated with stereotactic radiosurgery and dual CTLA-4/PD-1 blockade (ipilimumab/nivolumab), developed systemic disease progression and innumerable brain metastases. This patient achieved a complete CNS response and partial systemic response with standard whole brain radiation therapy (WBRT) combined with Talimogene laherparepvec (T-Vec) and pembrolizumab.
Conclusion: Patients who do not respond to one immunotherapy combination may respond during treatment with an alternate combination, even in the presence of multiple brain metastases. Biomarkers are needed to assist clinicians in evidence based clinical decision making after progression on first line immunotherapy to determine whether response can be achieved with second line immunotherapy.
Keywords: Anti-CTLA4; Anti-PD1; Brain metastases; Checkpoint inhibitors; Ipilimumab; Melanoma; Nivolumab; Pembrolizumab; T-Vec; Talimogene laherparepvec.
Conflict of interest statement
Ethics approval and consent to participate
Informed consent was obtained from our patient to enroll on a bio-specimen collection protocol (linked to a DataBase Shared Resource (DBSR) protocol) approved by the Columbia University Institutional Review Board.
Consent for publication
Informed consent was obtained from patient’s family for publication of patient history and images included in this submission as he is deceased at the time of authorship.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Response to the Rechallenge With Talimogene Laherparepvec (T-VEC) After Ipilimumab/Nivolumab Treatment in Patient With Cutaneous Malignant Melanoma Who Initially Had a Progression on T-VEC With Pembrolizumab.J Immunother. 2019 May;42(4):136-141. doi: 10.1097/CJI.0000000000000265. J Immunother. 2019. PMID: 30933044
-
Talimogene laherparepvec treatment to overcome loco-regional acquired resistance to immune checkpoint blockade in tumor stage IIIB-IV M1c melanoma patients.Cancer Immunol Immunother. 2020 May;69(5):759-769. doi: 10.1007/s00262-020-02487-x. Epub 2020 Feb 12. Cancer Immunol Immunother. 2020. PMID: 32052079 Free PMC article.
-
Metastatic melanoma in a 95 years old patient responding to treatment with talimogene laherparepvec followed by nivolumab.Acta Oncol. 2017 Oct;56(10):1327-1330. doi: 10.1080/0284186X.2017.1324212. Epub 2017 May 8. Acta Oncol. 2017. PMID: 28481677 No abstract available.
-
Unmasking of intracranial metastatic melanoma during ipilimumab/nivolumab therapy: case report and literature review.BMC Cancer. 2018 May 9;18(1):549. doi: 10.1186/s12885-018-4470-y. BMC Cancer. 2018. PMID: 29743050 Free PMC article. Review.
-
The safety of talimogene laherparepvec for the treatment of advanced melanoma.Expert Opin Drug Saf. 2017 Feb;16(2):265-269. doi: 10.1080/14740338.2017.1274729. Epub 2016 Dec 28. Expert Opin Drug Saf. 2017. PMID: 27989216 Review.
Cited by
-
Evaluating the efficacy of combination and single-agent immunotherapies in real-world patterns of disease progression and survival of metastatic melanoma patients.Melanoma Res. 2024 Apr 1;34(2):134-141. doi: 10.1097/CMR.0000000000000945. Epub 2024 Jan 4. Melanoma Res. 2024. PMID: 38181115 Free PMC article.
-
Emerging systemic delivery strategies of oncolytic viruses: A key step toward cancer immunotherapy.Nano Res. 2022;15(5):4137-4153. doi: 10.1007/s12274-021-4031-6. Epub 2022 Feb 14. Nano Res. 2022. PMID: 35194488 Free PMC article. Review.
-
New characteristics of cancer immunotherapy: trends in viral tumor immunotherapy with influenza virus-based approaches.J Zhejiang Univ Sci B. 2025 May 23;26(6):546-556. doi: 10.1631/jzus.B2400381. J Zhejiang Univ Sci B. 2025. PMID: 40571659 Free PMC article. Review.
-
Therapeutic vaccination immunomodulation: forming the basis of all cancer immunotherapy.Ther Adv Vaccines Immunother. 2019 Aug 1;7:2515135519862234. doi: 10.1177/2515135519862234. eCollection 2019. Ther Adv Vaccines Immunother. 2019. PMID: 31414074 Free PMC article. Review.
-
Radiation to all macroscopic sites of tumor permits greater systemic antitumor response to in situ vaccination.J Immunother Cancer. 2023 Jan;11(1):e005463. doi: 10.1136/jitc-2022-005463. J Immunother Cancer. 2023. PMID: 36639155 Free PMC article.
References
-
- Wolchok JD, Chiarion-Sileni V, Gonzalez R, et al. Updated results from a phase III trial of nivolumab (NIVO) combined with ipilimumab (IPI) in treatment-naive patients (pts) with advanced melanoma (MEL) (CheckMate 067) J Clin Oncol. 2016;34:9505.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical