

Efficacy and Safety of Apixaban, Dabigatran, Rivaroxaban, and Warfarin in Asians With Nonvalvular Atrial Fibrillation
- PMID: 29622587
- PMCID: PMC6015442
- DOI: 10.1161/JAHA.117.008150
Efficacy and Safety of Apixaban, Dabigatran, Rivaroxaban, and Warfarin in Asians With Nonvalvular Atrial Fibrillation
Abstract
Background: Whether non-vitamin K antagonist oral anticoagulants (NOACs) are superior to warfarin among Asians with nonvalvular atrial fibrillation remains unclear.
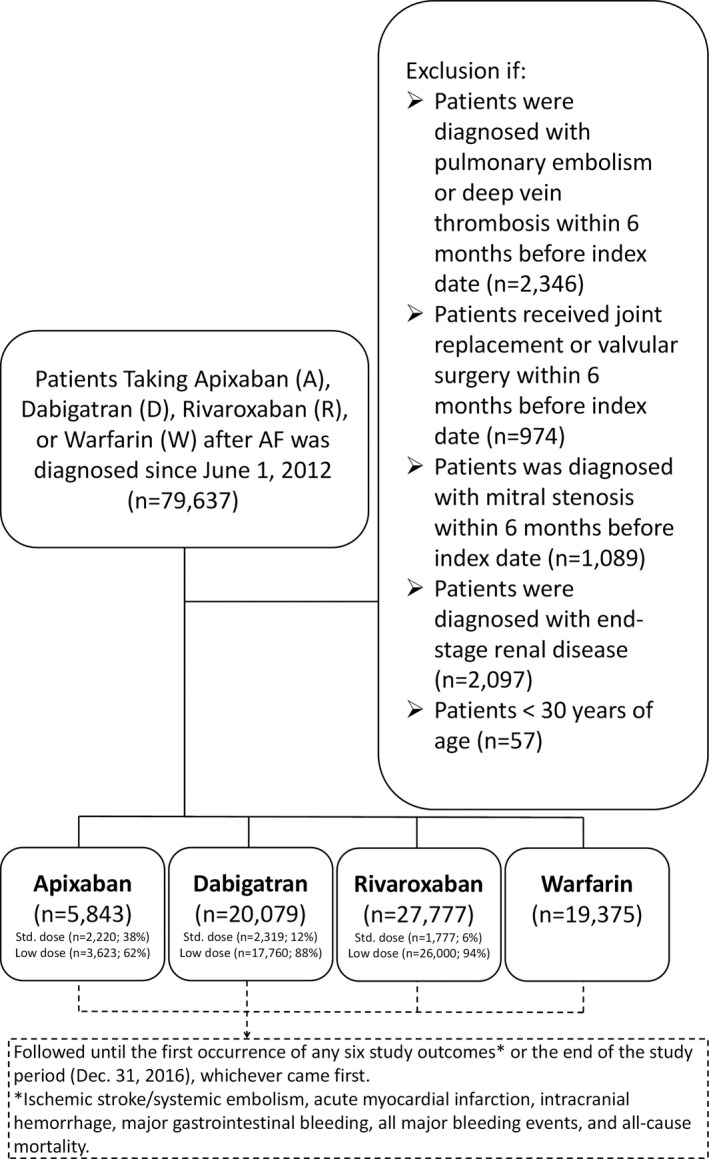
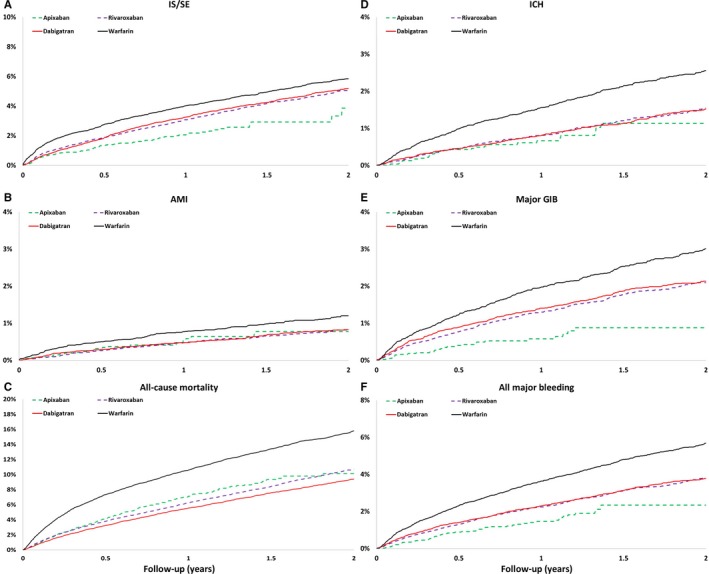
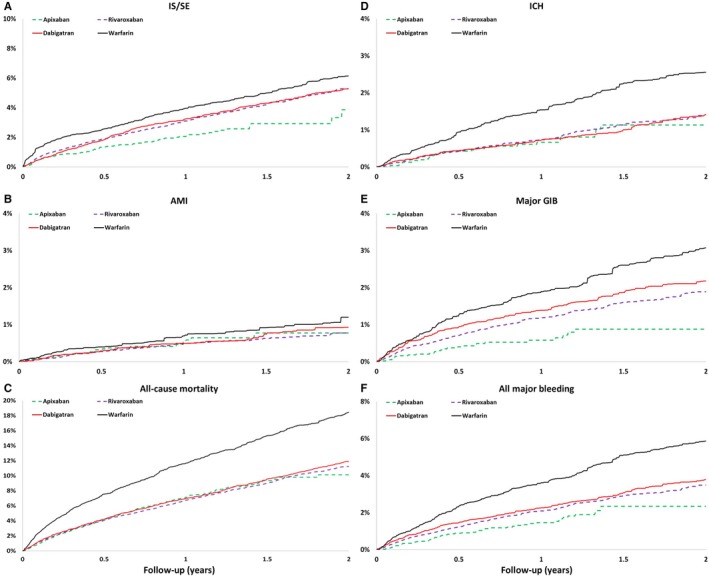
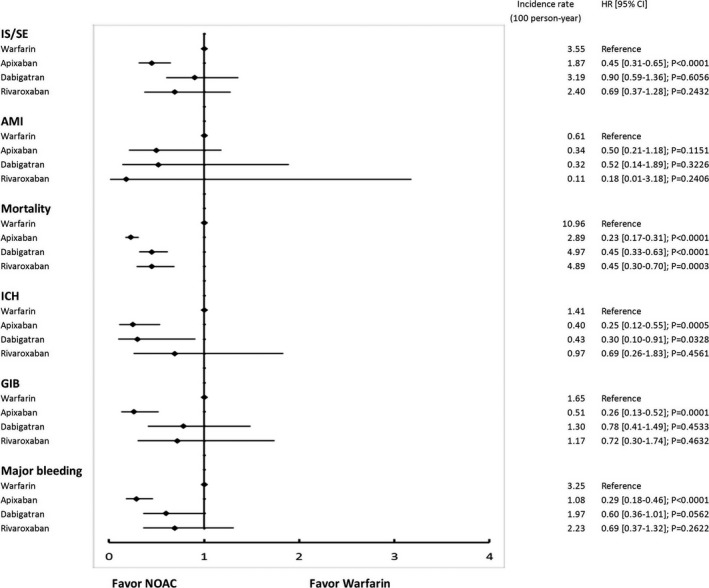
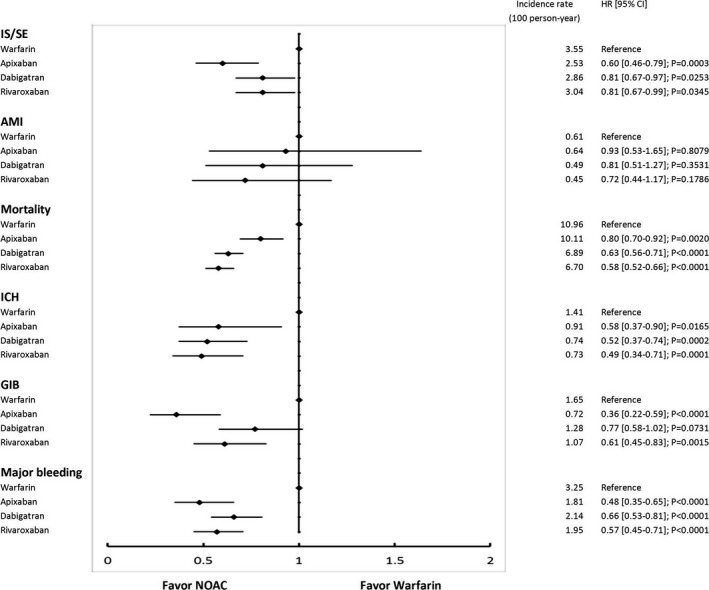
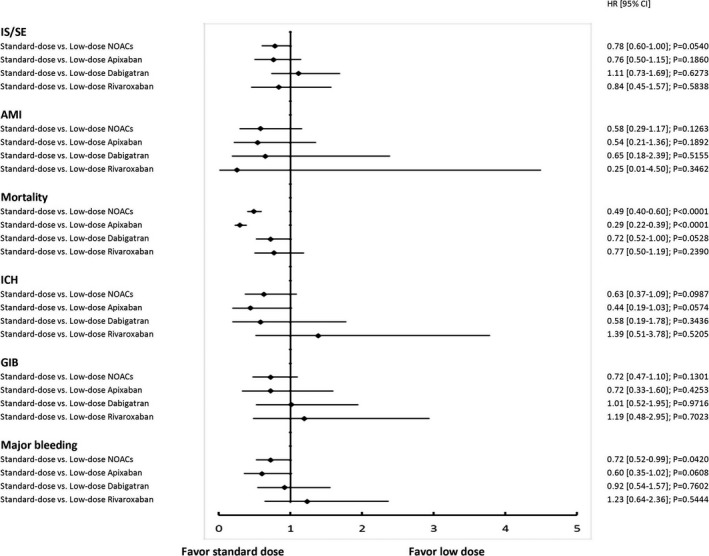
Methods and results: In this nationwide retrospective cohort study collected from Taiwan National Health Insurance Research Database, there were 5843, 20 079, 27 777, and 19 375 nonvalvular atrial fibrillation patients taking apixaban, dabigatran, rivaroxaban and warfarin, respectively, from June 1, 2012 to December 31, 2016. Propensity-score weighting was used to balance covariates across study groups. Patients were followed until the first occurrence of any efficacy or safety outcome or the end date of study. Hazard ratios (95% confidence intervals) comparing apixaban, dabigatran, and rivaroxaban with warfarin were: ischemic stroke/systemic embolism (IS/SE), 0.55 (0.43-0.69), 0.82 (0.68-0.98), and 0.81 (0.67-0.97); major bleeding, 0.41 (0.31-0.53), 0.65 (0.53-0.80), and 0.58 (0.46-0.72); and all-cause mortality, 0.58 (0.51-0.66), 0.61 (0.54-0.68), and 0.57 (0.51-0.65). A total of 3623 (62%), 17 760 (88%), and 26 000 (94%) patients were taking low-dose apixaban (2.5 mg twice daily), dabigatran (110 mg twice daily), and rivaroxaban (10-15 mg once daily), respectively. Similar to all-dose NOACs, all low-dose NOACs had lower risk of IS/SE, major bleeding, and mortality when compared with warfarin. In contrast to other standard-dose NOACs, apixaban was associated with lower risks of IS/SE (0.45 [0.31-0.65]), major bleeding (0.29 [0.18-0.46]), and mortality (0.23 [0.17-0.31]) than warfarin.
Conclusions: All NOACs were associated with lower risk of IS/SE, major bleeding, and mortality compared with warfarin in the largest real-world practice among Asians with nonvalvular atrial fibrillation. All low-dose NOACs had lower risk of IS/SE, major bleeding, and mortality when compared with warfarin. Standard-dose apixaban caused a lower risk of IS/SE, major bleeding, and mortality compared with warfarin.
Keywords: atrial fibrillation; direct thrombin inhibitor; factor Xa inhibitor; hemorrhage; ischemic stroke; mortality; warfarin.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures

References
-
- Chiang CE, Wu TJ, Ueng KC, Chao TF, Chang KC, Wang CC, Lin YJ, Yin WH, Kuo JY, Lin WS, Tsai CT, Liu YB, Lee KT, Lin LJ, Lin LY, Wang KL, Chen YJ, Chen MC, Cheng CC, Wen MS, Chen WJ, Chen JH, Lai WT, Chiou CW, Lin JL, Yeh SJ, Chen SA. 2016 guidelines of the Taiwan Heart Rhythm Society and the Taiwan Society of Cardiology for the management of atrial fibrillation. J Formos Med Assoc. 2016;115:893–952. - PubMed
-
- Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, Pogue J, Reilly PA, Themeles E, Varrone J, Wang S, Alings M, Xavier D, Zhu J, Diaz R, Lewis BS, Darius H, Diener HC, Joyner CD, Wallentin L; Committee R‐LS, Investigators . Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139–1151. - PubMed
-
- Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, Breithardt G, Halperin JL, Hankey GJ, Piccini JP, Becker RC, Nessel CC, Paolini JF, Berkowitz SD, Fox KA, Califf RM; ROCKET AF Investigators . Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883–891. - PubMed
-
- Granger CB, Alexander JH, McMurray JJ, Lopes RD, Hylek EM, Hanna M, Al‐Khalidi HR, Ansell J, Atar D, Avezum A, Bahit MC, Diaz R, Easton JD, Ezekowitz JA, Flaker G, Garcia D, Geraldes M, Gersh BJ, Golitsyn S, Goto S, Hermosillo AG, Hohnloser SH, Horowitz J, Mohan P, Jansky P, Lewis BS, Lopez‐Sendon JL, Pais P, Parkhomenko A, Verheugt FW, Zhu J, Wallentin L; ARISTOTLE Committees and Investigators . Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981–992. - PubMed
-
- Giugliano RP, Ruff CT, Braunwald E, Murphy SA, Wiviott SD, Halperin JL, Waldo AL, Ezekowitz MD, Weitz JI, Spinar J, Ruzyllo W, Ruda M, Koretsune Y, Betcher J, Shi M, Grip LT, Patel SP, Patel I, Hanyok JJ, Mercuri M, Antman EM; ENGAGE AF‐TIMI Investigators . Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369:2093–2104. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
