

Immune-related endocrine disorders in novel Immune checkpoint inhibition therapy
- PMID: 29623291
- PMCID: PMC5881952
- DOI: 10.1016/j.gendis.2016.10.002
Immune-related endocrine disorders in novel Immune checkpoint inhibition therapy
Abstract
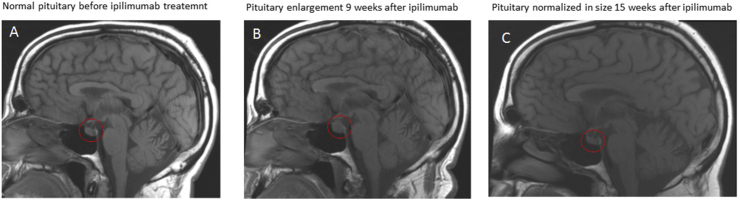
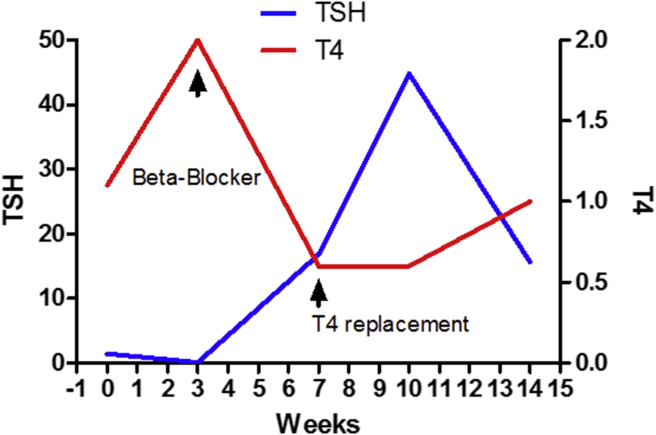
Immune checkpoint inhibition against advance malignancies was named breakthrough discovery by the science magazine in 2013. In numerous clinical studies, monoclonal antibodies against the immune checkpoints, CTLA4, PD1 and PD1 ligand PDL1 have shown promising tumor response in different type of metastatic malignancies. The adverse events are autoimmune-related. The endocrine disorders, hypothysitis and thyroiditis are among the most common side effects associated with immune checkpoint inhibition treatment. Hypophysitis, a very rare endocrine disorder occurs in about one tenth of the patients receiving anti-CTLA4 treatment. Thyroiditis, on the other hand, is more commonly seen in patients receiving anti-PD1 treatment. In addition, both thyroiditis and hypophysitis are common in patients receiving combination treatment with anti-CTLA4 and anti-PD1 treatment. The time to onset of hypophysitis and thyroiditis is short. Most of the endocrine disorders occur within 12 weeks after initiation of the immune checkpoint inhibition therapy. Hypohysitis can manifest as total anterior pituitary hormone deficiency or isolated pituitary hormone deficiency. Diabetes insipidus is rare. TSH and gonadotropin deficiencies may be reversible but ACTH deficiency appears permanent. Thyroiditis can present as hypothyroidism or thyrotoxicosis followed by hypothyroidism. Hypothyroidism appears irreversible. Early identifying the onset of hypophysitis and thyroiditis and proper management of these endocrine disorders will improve the quality of the life and the outcome of this novel immunotherapy.
Figures
References
-
- Khattri R., Auger J.A., Griffin M.D., Sharpe A.H., Bluestone J.A. Lymphoproliferative disorder in CTLA-4 knockout mice is characterized by CD28-regulated activation of Th2 responses. J Immunol. 1999;162(10):5784–5791. - PubMed
-
- Nishimura H., Minato N., Nakano T., Honjo T. Immunological studies on PD-1 deficient mice: implication of PD-1 as a negative regulator for B cell responses. Int Immunol. 1998;10(10):1563–1572. - PubMed
-
- Parish C.R. Cancer immunotherapy: the past, the present and the future. Immunol Cell Biol. 2003;81(2):106–113. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials