

Gender Differences in Clinical Outcomes after Catheter Ablation of Atrial Fibrillation
- PMID: 29623299
- PMCID: PMC5881580
- DOI: 10.1016/j.jacep.2016.04.014
Gender Differences in Clinical Outcomes after Catheter Ablation of Atrial Fibrillation
Abstract
Objective: To explore gender differences in real-world outcomes after catheter ablation of atrial fibrillation (AF).
Background: Compared to men, women with AF have greater thromboembolic risk and tend to be more symptomatic. Catheter ablation is generally more effective than antiarrhythmic drug therapy alone. However, there is limited data on the influence of gender on AF ablation outcomes.
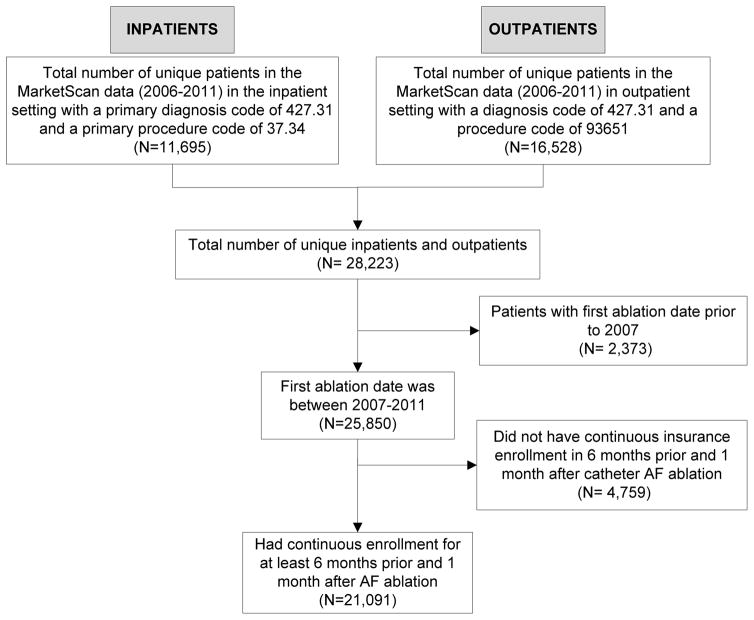
Methods: We analyzed medical claims of 45 million United States patients enrolled in a variety of employee-sponsored and fee-for-service plans. We identified patients who underwent an AF ablation from 2007 to 2011 and evaluated 30-day safety and one-year effectiveness outcomes.
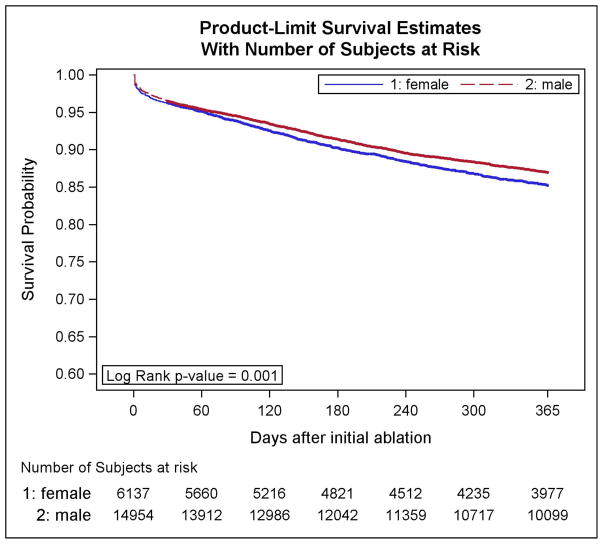
Results: Of the 21,091 patients who underwent an AF ablation, 7,460 (29%) were female. Women, compared to men, were older (62±11 vs. 58±11 years), had higher CHADS2 (1.2±1.1 vs. 1.0±1.0), higher CHA2DS2-VASc (2.9±1.5 vs. 1.6±1.4), and higher Charlson comorbidity index scores (1.2±1.3 vs. 1.0±1.2)(p<0.001 for all). Following ablation, women had higher risk of 30-day complications of hemorrhage (2.7 vs. 2.0%,p<0.001) and tamponade (3.8 vs. 2.9%,p<0.001). In multivariable analyses, women were more likely to have a re-hospitalization for AF (adjusted HR 1.12,p=0.009), but less likely to have repeat AF ablation (adjusted HR 0.92,p=0.04) or cardioversion (adjusted HR 0.75,p<0.001).
Conclusion: Women have increased hospitalization rates after AF ablation and are more likely to have a procedural complication. Despite the higher rate of hospital admissions for AF after ablation, women were less likely to undergo repeat ablation or cardioversion. These data call for greater examination of barriers and facilitators to sustain rhythm control strategies in women.
Keywords: atrial fibrillation; catheter ablation; disparities; rhythm control; women.
Conflict of interest statement
Disclosures: There are no conflicts of interest to report.
Figures
References
-
- Lloyd-Jones DM, Wang TJ, Leip EP, et al. Lifetime risk for development of atrial fibrillation: the Framingham Heart Study. Circulation. 2004;110:1042–6. - PubMed
-
- January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130:2071–104. - PubMed
-
- Suttorp MJ, Kingma JH, Koomen EM, van 't Hof A, Tijssen JG, Lie KI. Recurrence of paroxysmal atrial fibrillation or flutter after successful cardioversion in patients with normal left ventricular function. The American journal of cardiology. 1993;71:710–3. - PubMed
-
- Van Gelder IC, Hagens VE, Bosker HA, et al. A comparison of rate control and rhythm control in patients with recurrent persistent atrial fibrillation. The New England journal of medicine. 2002;347:1834–40. - PubMed
-
- Rienstra M, Van Veldhuisen DJ, Hagens VE, et al. Gender-related differences in rhythm control treatment in persistent atrial fibrillation: data of the Rate Control Versus Electrical Cardioversion (RACE) study. Journal of the American College of Cardiology. 2005;46:1298–306. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous