

Visual field deficits after epilepsy surgery: a new quantitative scoring method
- PMID: 29623432
- PMCID: PMC5995984
- DOI: 10.1007/s00701-018-3525-9
Visual field deficits after epilepsy surgery: a new quantitative scoring method
Abstract
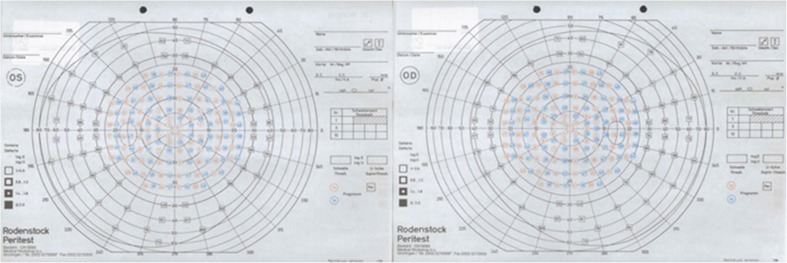
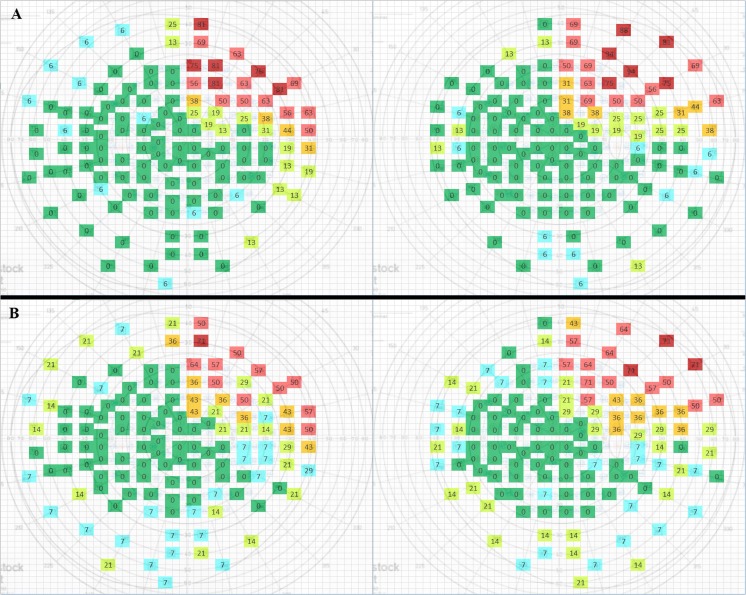
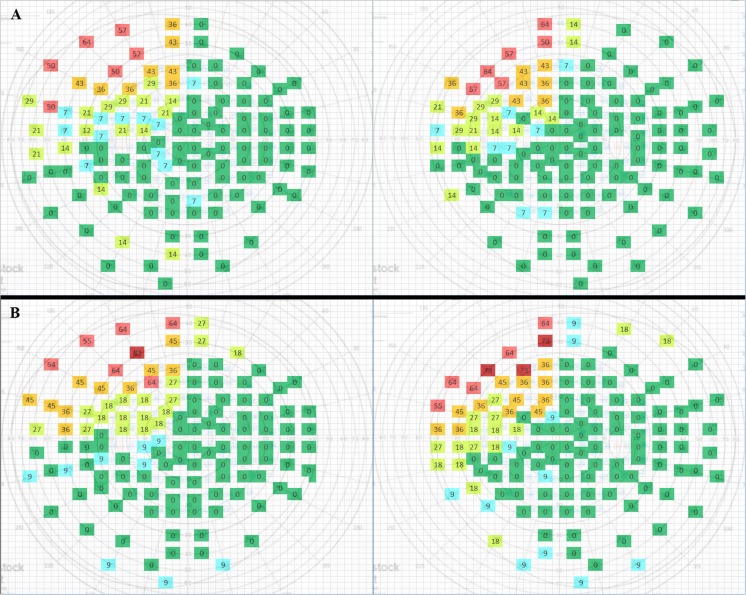
Background: Anterior temporal lobectomy (ATL) as a treatment for drug-resistant temporal lobe epilepsy (TLE) frequently causes visual field deficits (VFDs). Reported VFD encompasses homonymous contralateral upper quadrantanopia. Its reported incidence ranges from 15 to 90%. To date, a quantitative method to evaluate postoperative VFD in static perimetry is not available. A method to quantify postoperative VFD, which allows for comparison between groups of patients, was developed.
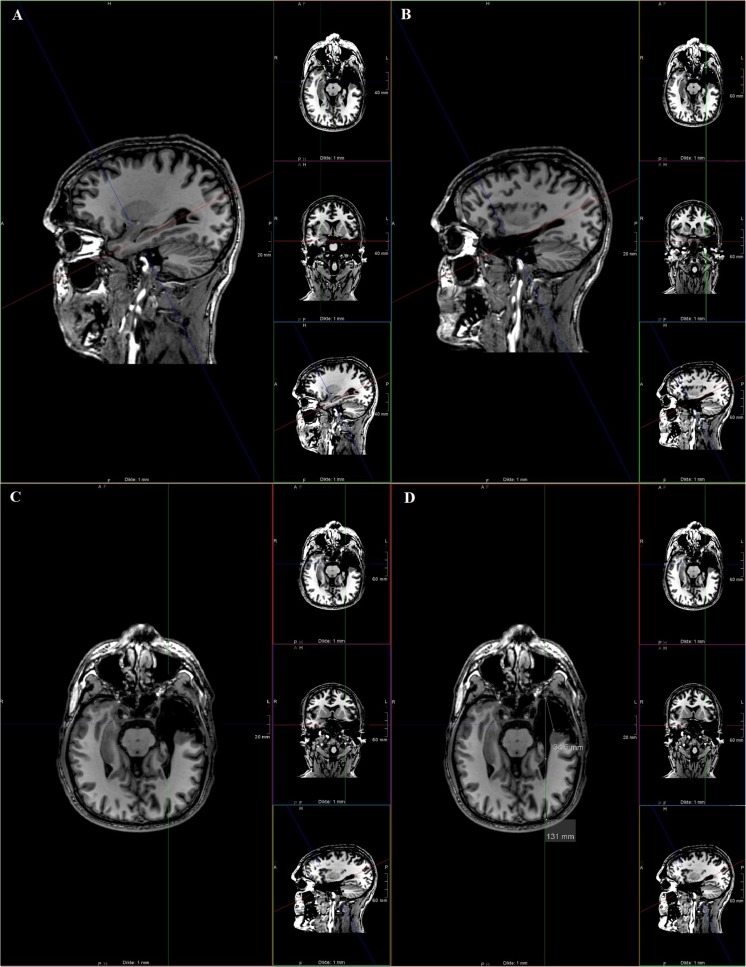
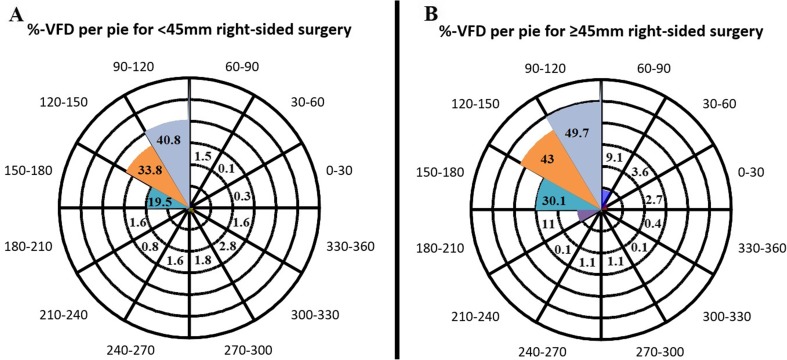
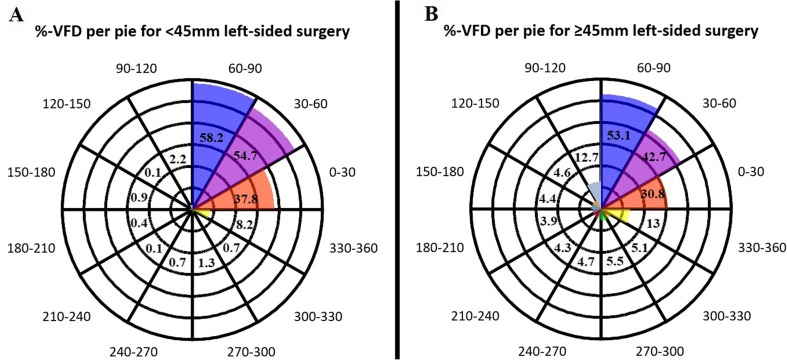
Methods: Fifty-five patients with drug-resistant TLE, who underwent ATL with pre- and postoperative perimetry, were included. Temporal lobe resection length was measured on postoperative MRI. Percentage VFD was calculated for the total visual field, contralateral upper quadrant, or other three quadrants combined.
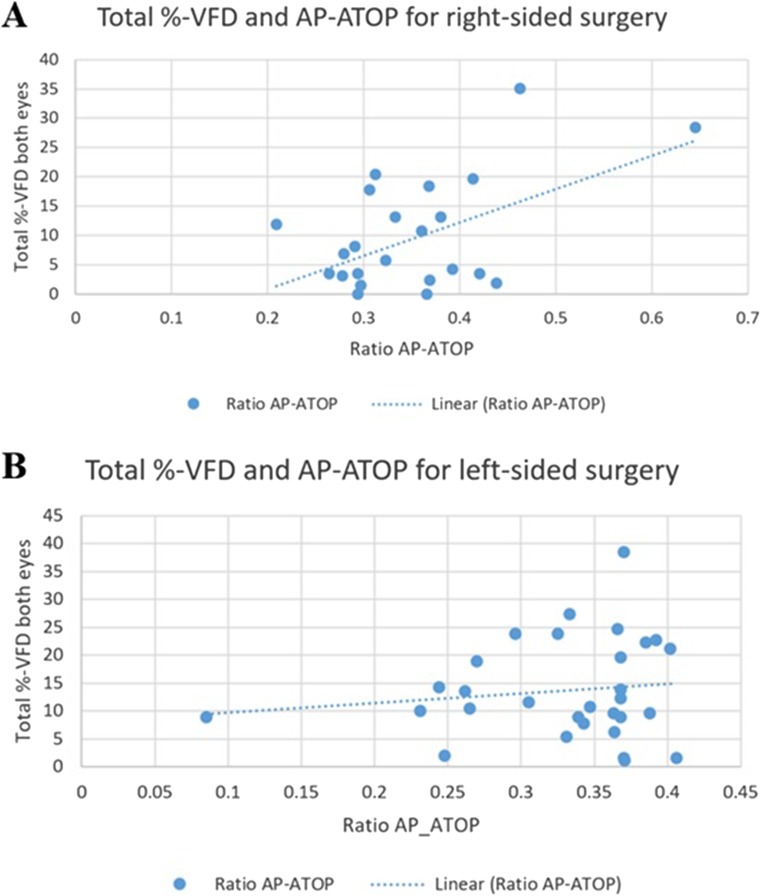
Results: Patients were divided into groups by resection size (< 45 and ≥ 45 mm) and side of surgery (right and left). We found significant higher VFD in the ≥ 45 vs. < 45 mm group (2.3 ± 4.4 vs. 0.7 ± 2.4%,p = 0.04) for right-sided ATL. Comparing VFD in both eyes, we found more VFD in the right vs. left eye following left-sided ATL (14.5 ± 9.8 vs. 12.9 ± 8.3%, p = 0.03). We also demonstrated significantly more VFD in the < 45 mm group for left- vs. right-sided surgery (6.7 ± 6.7 vs. 13.1 ± 7.0%, p = 0.016). A significant quantitative correlation between VFD and resection size for right-sided ATL was shown (r = 0.52, p < 0.01).
Conclusions: We developed a new quantitative scoring method for the assessment of postoperative visual field deficits after temporal lobe epilepsy surgery and assessed its feasibility for clinical use. A significant correlation between VFD and resection size for right-sided ATL was confirmed.
Keywords: Epilepsy; Perimetry; Quadrantanopia; Temporal lobectomy; Visual field deficits.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures
References
-
- CBR, "Centraal Bureau Rijvaardigheidsbewijzen," CBR 2017. [Online]. Available: https://www.cbr.nl/oogaandoening.pp. [Accessed 30 May 2017]
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
