

First-in-human intraoperative near-infrared fluorescence imaging of glioblastoma using cetuximab-IRDye800
- PMID: 29623552
- PMCID: PMC6031450
- DOI: 10.1007/s11060-018-2854-0
First-in-human intraoperative near-infrared fluorescence imaging of glioblastoma using cetuximab-IRDye800
Abstract
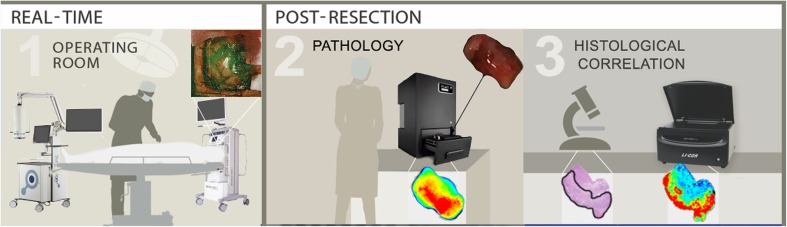
Introduction: Maximizing extent of surgical resection with the least morbidity remains critical for survival in glioblastoma patients, and we hypothesize that it can be improved by enhancements in intraoperative tumor detection. In a clinical study, we determined if therapeutic antibodies could be repurposed for intraoperative imaging during resection.
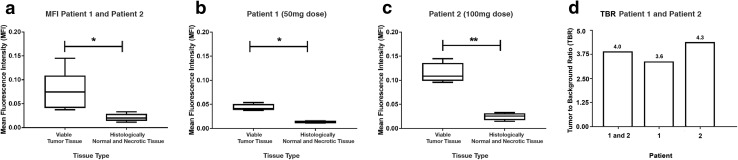
Methods: Fluorescently labeled cetuximab-IRDye800 was systemically administered to three patients 2 days prior to surgery. Near-infrared fluorescence imaging of tumor and histologically negative peri-tumoral tissue was performed intraoperatively and ex vivo. Fluorescence was measured as mean fluorescence intensity (MFI), and tumor-to-background ratios (TBRs) were calculated by comparing MFIs of tumor and histologically uninvolved tissue.
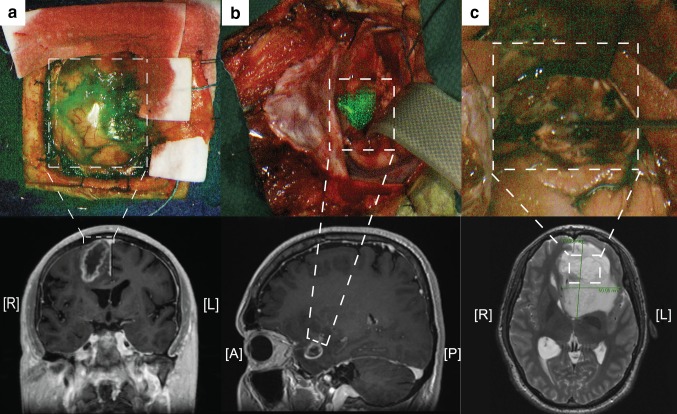
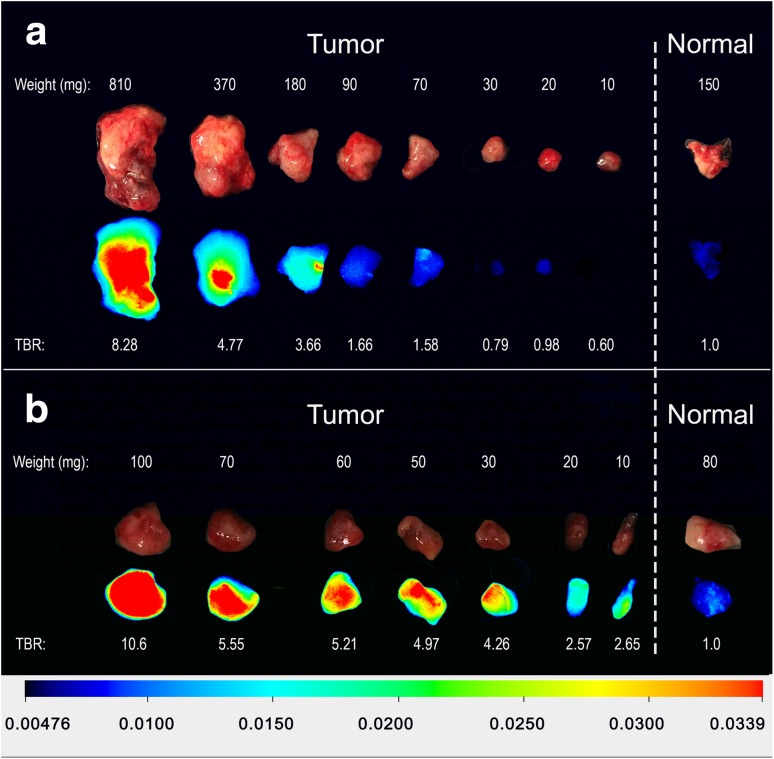
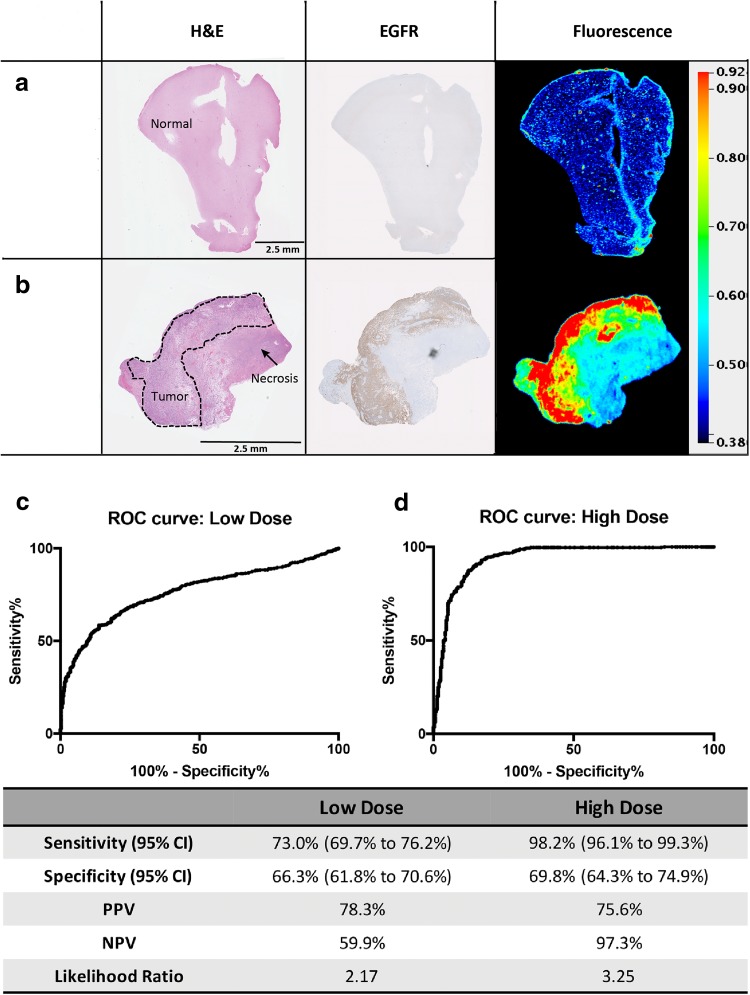
Results: The mean TBR was significantly higher in tumor tissue of contrast-enhancing (CE) tumors on preoperative imaging (4.0 ± 0.5) compared to non-CE tumors (1.2 ± 0.3; p = 0.02). The TBR was higher at a 100 mg dose than at 50 mg (4.3 vs. 3.6). The smallest detectable tumor volume in a closed-field setting was 70 mg with 50 mg of dye and 10 mg with 100 mg. On sections of paraffin embedded tissues, fluorescence positively correlated with histological evidence of tumor. Sensitivity and specificity of tumor fluorescence for viable tumor detection was calculated and fluorescence was found to be highly sensitive (73.0% for 50 mg dose, 98.2% for 100 mg dose) and specific (66.3% for 50 mg dose, 69.8% for 100 mg dose) for viable tumor tissue in CE tumors while normal peri-tumoral tissue showed minimal fluorescence.
Conclusion: This first-in-human study demonstrates the feasibility and safety of antibody based imaging for CE glioblastomas.
Keywords: Antibody-based imaging; Brain neoplasms; Cetuximab; Fluorescence; Glioblastoma; Image-guided surgery; Phase 1.
Conflict of interest statement
The authors have no relevant conflicts of interest to disclose.
Figures
References
-
- Nimsky C, Ganslandt O, Cerny S, Hastreiter P, Greiner G, Fahlbusch R (2000) Quantification of, visualization of, and compensation for brain shift using intraoperative magnetic resonance imaging. Neurosurgery 47(5):1070–1079. http://www.ncbi.nlm.nih.gov/pubmed/11063099. Accessed 16 Oct 2017 - PubMed
-
- Cortnum S, Laursen RJ (2012) Fluorescence-guided resection of gliomas. Dan Med J 59(8):A4460. http://www.ncbi.nlm.nih.gov/pubmed/22849976. Accessed 16 Oct 2017 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
