

Trajectories of Depressive Symptoms Among a Population of HIV-Infected Men and Women in Routine HIV Care in the United States
- PMID: 29623578
- PMCID: PMC6423517
- DOI: 10.1007/s10461-018-2109-2
Trajectories of Depressive Symptoms Among a Population of HIV-Infected Men and Women in Routine HIV Care in the United States
Abstract
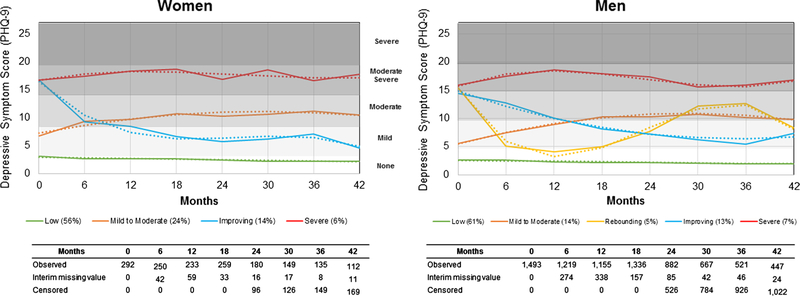
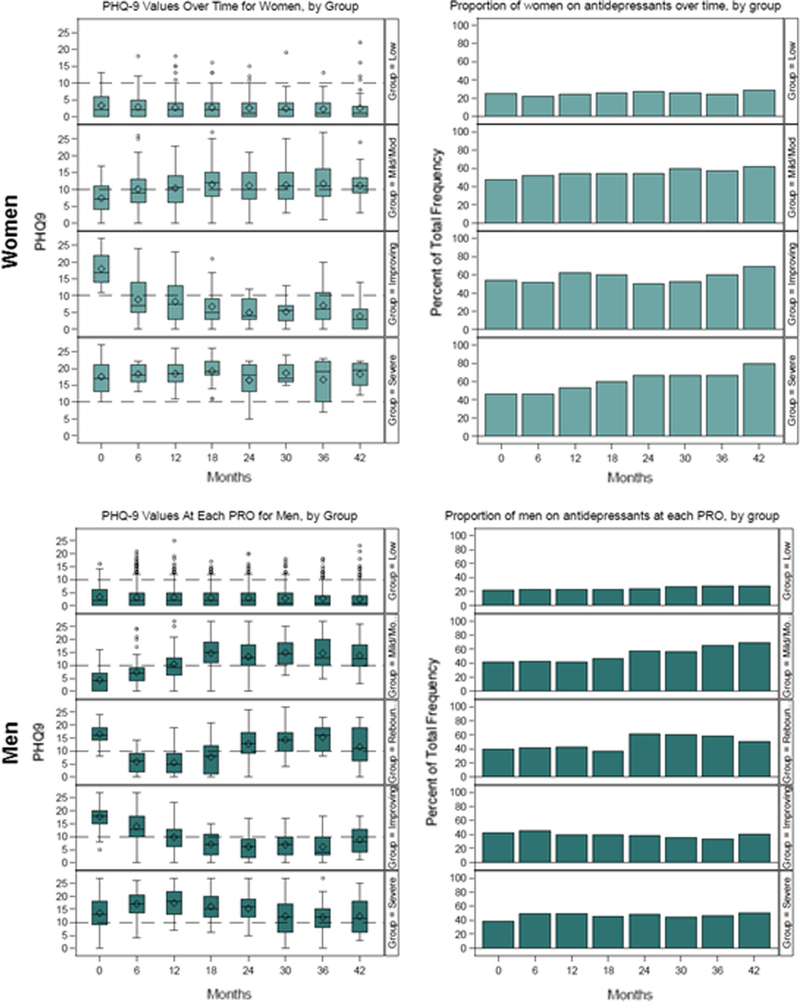
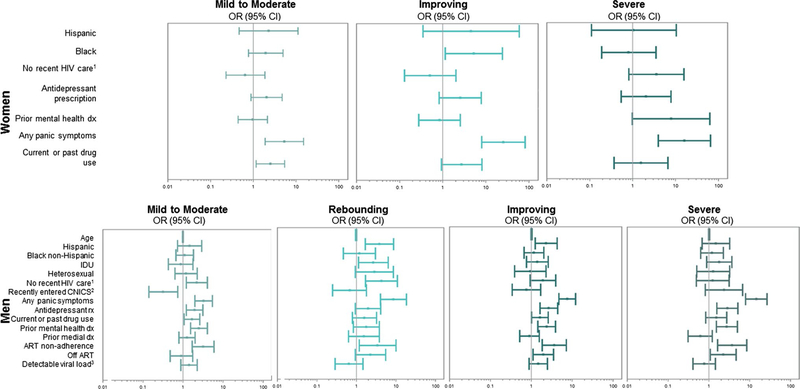
Depressive symptoms vary in severity and chronicity. We used group-based trajectory models to describe trajectories of depressive symptoms (measured using the Patient Health Questionnaire-9) and predictors of trajectory group membership among 1493 HIV-infected men (84%) and 292 HIV-infected women (16%). At baseline, 29% of women and 26% of men had depressive symptoms. Over a median of 30 months of follow-up, we identified four depressive symptom trajectories for women (labeled "low" [experienced by 56% of women], "mild/moderate" [24%], "improving" [14%], and "severe" [6%]) and five for men ("low" [61%], "mild/moderate" [14%], "rebounding" [5%], "improving" [13%], and "severe" [7%]). Baseline antidepressant prescription, panic symptoms, and prior mental health diagnoses were associated with more severe or dynamic depressive symptom trajectories. Nearly a quarter of participants experienced some depressive symptoms, highlighting the need for improved depression management. Addressing more severe or dynamic depressive symptom trajectories may require interventions that additionally address mental health comorbidities.
Keywords: Depression; Depressive symptoms; Group-based trajectory models; HIV; Trajectory analysis.
Conflict of interest statement
Figures
References
-
- Bing EG, Burnam MA, Longshore D, Fleishman JA, Sherbourne CD, London AS, et al. Psychiatric disorders and drug use among human immunodeficiency virus-infected adults in the United States. Arch Gen Psychiatry. 2001;58(8):721–8. - PubMed
-
- Ciesla JA, Roberts JE. Meta-analysis of the relationship between HIV infection and risk for depressive disorders. Am J Psychiatry. 2001;158(5):725–30. - PubMed
-
- Zimpel RR, Fleck MP. Depression as a major impact on the quality of life of HIV-positive Brazilians. Psychol Health Med. 2014;19(1):47–58. - PubMed
MeSH terms
Grants and funding
- R01 MH100970/MH/NIMH NIH HHS/United States
- L30 MH110572/MH/NIMH NIH HHS/United States
- UL1 TR001111/TR/NCATS NIH HHS/United States
- UL1TR001111/National Institutes of Health
- P30 AI50410/National Institute of Allergy and Infectious Diseases
- R24AI067039/National Institute of Allergy and Infectious Diseases
- L30MH110572/National Institute of Mental Health
- R24 AI067039/AI/NIAID NIH HHS/United States
- K99 MH112413/MH/NIMH NIH HHS/United States
- R01MH100970/National Institute of Mental Health
- K99MH112413/National Institute of Mental Health
- P30 AI050410/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
