

Healthcare Cost Development in a Type 2 Diabetes Patient Population on Glucose-Lowering Drug Treatment: A Nationwide Observational Study 2006-2014
- PMID: 29623637
- PMCID: PMC6249189
- DOI: 10.1007/s41669-017-0063-y
Healthcare Cost Development in a Type 2 Diabetes Patient Population on Glucose-Lowering Drug Treatment: A Nationwide Observational Study 2006-2014
Abstract
Objective: The objective of this study was to describe healthcare resource use and cost development in Sweden during 2006-2014 in a type 2 diabetes (T2D) population receiving glucose-lowering drugs (GLDs).
Methods: In- and outpatient healthcare resource use and costs were extracted from mandatory national registries: the Cause of Death Register; the National Patient Register; and the Prescribed Drug Register. Primary care data were estimated based on an observational study including patients from 84 primary care centers in Sweden. Numbers of any cause inpatient, outpatient, and primary care contacts were extracted and direct healthcare costs were estimated.
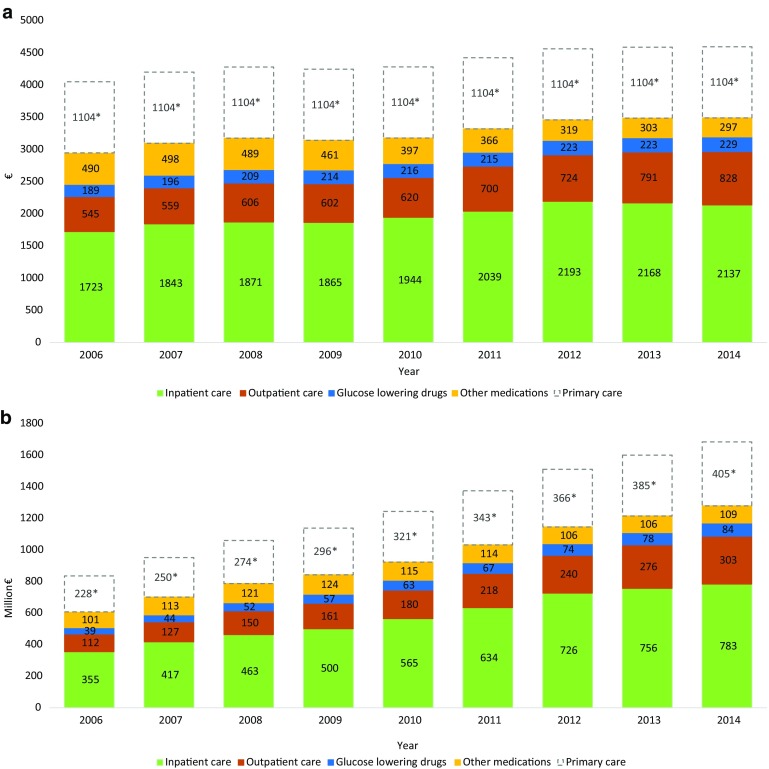
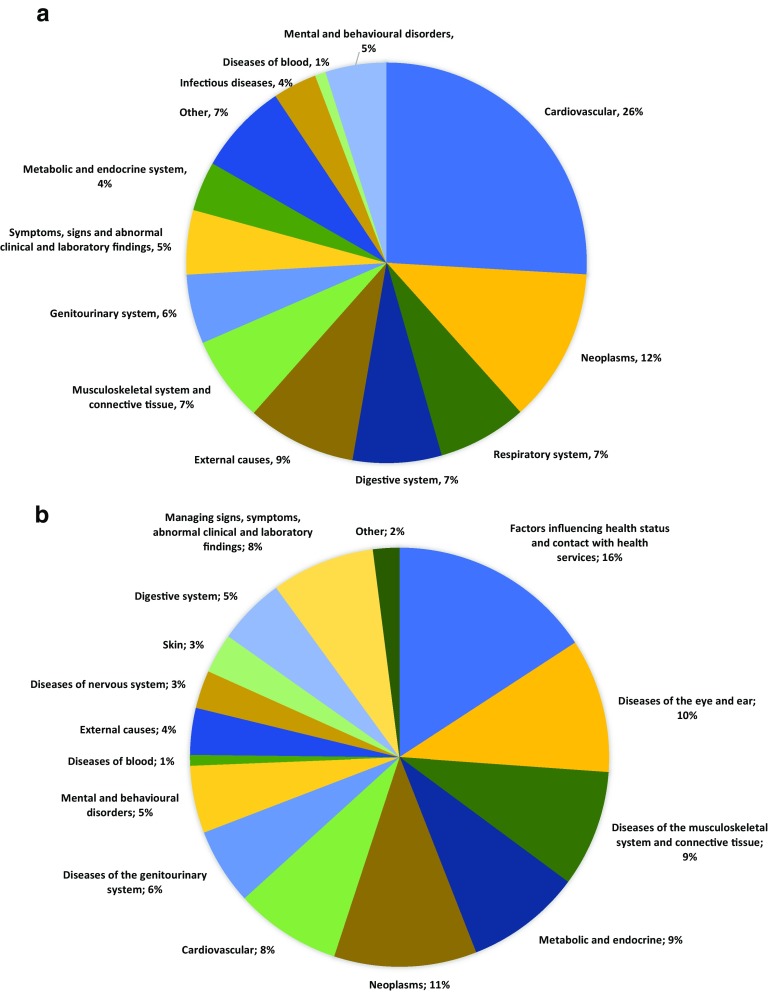
Results: During 2006-2014, the number of inpatient and primary care contacts increased by approximately 70% (from 45,559 to 78,245 and from 4.9 to 8.8 million, respectively) and outpatient care contacts almost doubled (from 105,653 to 209,417). Mean annual per patient costs increased by 13%, reaching €4594. Total healthcare costs increased from €835 million to €1.684 billion. Inpatient care costs constituted 47% of total costs in 2014 (€783 million), primary care accounted for 24% (€405 million), outpatient care 18% (€303 million), non-GLD medications 6% (€109 million), and GLDs 5% (€84 million). Cardiovascular diseases (CVDs) were the most costly disease group in inpatient care (26%), whereas managing unspecified factors influencing health and T2D-associated diseases were the most costly in outpatient care (16 and 11%, respectively).
Conclusions: The healthcare costs of the GLD-treated T2D population doubled during 2006-2014, mostly driven by the increasing size of this population, of which inpatient care accounted for 47%. GLDs constituted the smallest share of costs. CVD was the most resource-requiring disease group.
Conflict of interest statement
US and JB hold full-time positions at AstraZeneca. DN, JWE, TN, AN, and UO have received compensation for their work from AstraZeneca.
Figures
References
-
- International Diabetes Federation. IDF diabetes atlas. 2014. http://www.diabetesatlas.org/. Accessed 15 May 2017.
-
- WHO. Global report of diabetes. Geneva: WHO; 2016. http://apps.who.int/iris/bitstream/10665/204871/1/9789241565257_eng.pdf. Accessed 15 May 2017.
-
- Norhammar A, Bodegard J, Nystrom T, Thuresson M, Eriksson JW, Nathanson D. Incidence, prevalence and mortality of type 2 diabetes requiring glucose-lowering treatment, and associated risks of cardiovascular complications: a nationwide study in Sweden, 2006–2013. Diabetologia. 2016;59(8):1692–1701. doi: 10.1007/s00125-016-3971-y. - DOI - PubMed
-
- Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ (Clin Res Ed). 2000;321(7258):405–412. doi: 10.1136/bmj.321.7258.405. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
