

Four-Gene Pan-African Blood Signature Predicts Progression to Tuberculosis
- PMID: 29624071
- PMCID: PMC6019933
- DOI: 10.1164/rccm.201711-2340OC
Four-Gene Pan-African Blood Signature Predicts Progression to Tuberculosis
Abstract
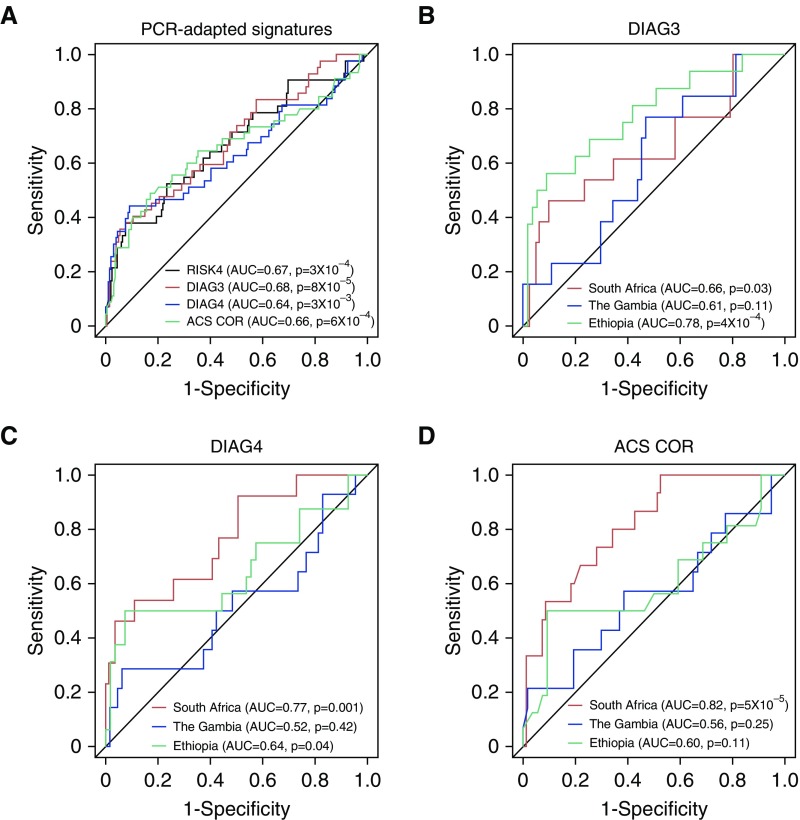
Rationale: Contacts of patients with tuberculosis (TB) constitute an important target population for preventive measures because they are at high risk of infection with Mycobacterium tuberculosis and progression to disease.Objectives: We investigated biosignatures with predictive ability for incident TB.Methods: In a case-control study nested within the Grand Challenges 6-74 longitudinal HIV-negative African cohort of exposed household contacts, we employed RNA sequencing, PCR, and the pair ratio algorithm in a training/test set approach. Overall, 79 progressors who developed TB between 3 and 24 months after diagnosis of index case and 328 matched nonprogressors who remained healthy during 24 months of follow-up were investigated.Measurements and Main Results: A four-transcript signature derived from samples in a South African and Gambian training set predicted progression up to two years before onset of disease in blinded test set samples from South Africa, the Gambia, and Ethiopia with little population-associated variability, and it was also validated in an external cohort of South African adolescents with latent M. tuberculosis infection. By contrast, published diagnostic or prognostic TB signatures were predicted in samples from some but not all three countries, indicating site-specific variability. Post hoc meta-analysis identified a single gene pair, C1QC/TRAV27 (complement C1q C-chain / T-cell receptor-α variable gene 27) that would consistently predict TB progression in household contacts from multiple African sites but not in infected adolescents without known recent exposure events.Conclusions: Collectively, we developed a simple whole blood-based PCR test to predict TB in recently exposed household contacts from diverse African populations. This test has potential for implementation in national TB contact investigation programs.
Keywords: biomarkers; gene expression; tuberculosis.
Figures




Comment in
-
Diagnostic Test for Incipient Tuberculosis: A Step Forward, Many More to Go.Am J Respir Crit Care Med. 2018 May 1;197(9):1106-1107. doi: 10.1164/rccm.201803-0469ED. Am J Respir Crit Care Med. 2018. PMID: 29624073 No abstract available.
References
-
- Riley F. Tuberculosis in hospital nurses; five years figures. Mon Bull Minist Health Public Health Lab Serv. 1959;18:38–45. - PubMed
-
- Yates TA, Khan PY, Knight GM, Taylor JG, McHugh TD, Lipman M, et al. The transmission of Mycobacterium tuberculosis in high burden settings. Lancet Infect Dis. 2016;16:227–238. - PubMed
-
- World Health Organization (WHO) Global tuberculosis report 2017. [accessed 2018 Jan 26]. Available from: http://www.who.int/tb/publications/global_report/gtbr2017_main_text.pdf?....
-
- Rieder H. Annual risk of infection with Mycobacterium tuberculosis. Eur Respir J. 2005;25:181–185. - PubMed
-
- O’Garra A, Redford PS, McNab FW, Bloom CI, Wilkinson RJ, Berry MP. The immune response in tuberculosis. Annu Rev Immunol. 2013;31:475–527. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
