

Paracetamol (acetaminophen) for patent ductus arteriosus in preterm or low birth weight infants
- PMID: 29624206
- PMCID: PMC6494526
- DOI: 10.1002/14651858.CD010061.pub3
Paracetamol (acetaminophen) for patent ductus arteriosus in preterm or low birth weight infants
Update in
-
Paracetamol (acetaminophen) for patent ductus arteriosus in preterm or low birth weight infants.Cochrane Database Syst Rev. 2020 Jan 27;1(1):CD010061. doi: 10.1002/14651858.CD010061.pub4. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2022 Dec 15;12:CD010061. doi: 10.1002/14651858.CD010061.pub5. PMID: 31985831 Free PMC article. Updated.
Abstract
Background: In preterm newborns, the ductus arteriosus frequently fails to close and the infants require medical or surgical closure of the patent ductus arteriosus (PDA). A PDA can be treated surgically; or medically with one of two prostaglandin inhibitors, indomethacin or ibuprofen. Case reports suggest that paracetamol may be an alternative for the closure of a PDA. An association between prenatal or postnatal exposure to paracetamol and later development of autism or autism spectrum disorder has been reported.
Objectives: To determine the effectiveness and safety of intravenous or oral paracetamol compared with placebo or no intervention, intravenous indomethacin, intravenous or oral ibuprofen, or with other cyclo-oxygenase inhibitors for treatment of an echocardiographically diagnosed PDA in preterm or low birth weight infants.
Search methods: We used the standard search strategy of Cochrane Neonatal to search the Cochrane Central Register of Controlled Trials (CENTRAL 2017, Issue 10), MEDLINE via PubMed (1966 to 6 November 2017), Embase (1980 to 6 November 2017), and CINAHL (1982 to 6 November 2017). We searched clinical trial databases, conference proceedings, and the reference lists of retrieved articles for randomised controlled trials (RCT) and quasi-randomised trials.
Selection criteria: We included RCTs in which paracetamol was compared to no intervention, placebo or other agents used for closure of PDA irrespective of dose, duration and mode of administration in preterm (≤ 34 weeks' postmenstrual age) infants. We both reviewed the search results and made a final selection of potentially eligible articles by discussion. We included studies of both prophylactic and therapeutic use of paracetamol.
Data collection and analysis: We performed data collection and analyses in accordance with the methods of the Cochrane Neonatal Review Group. We used the GRADE approach to assess the quality of evidence for the following outcomes when data were available: failure of ductal closure after the first course of treatment; neurodevelopmental impairment; all-cause mortality during initial hospital stay (death); gastrointestinal bleed or stools positive for occult blood; and serum levels of creatinine after treatment (µmol/L).
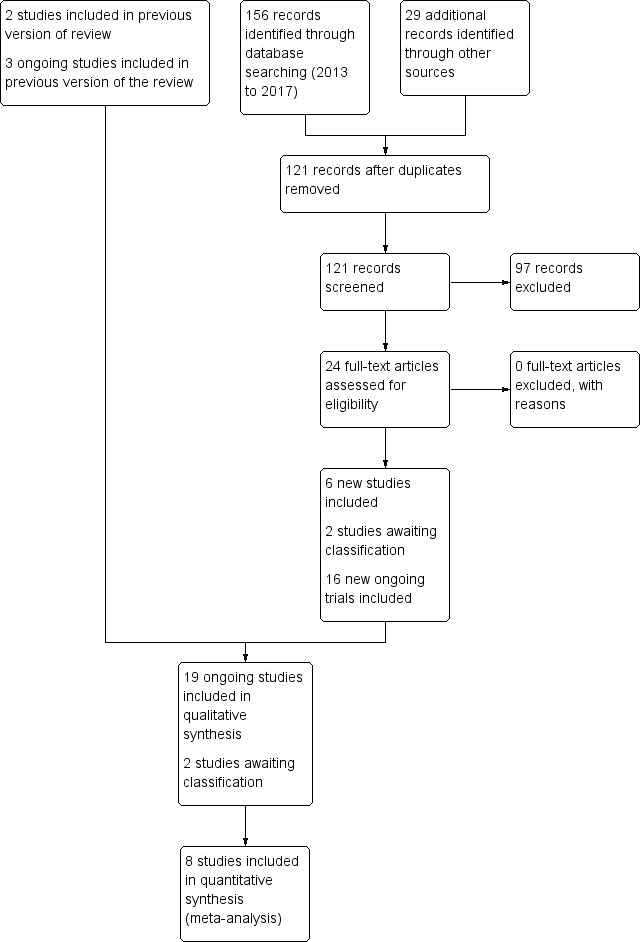
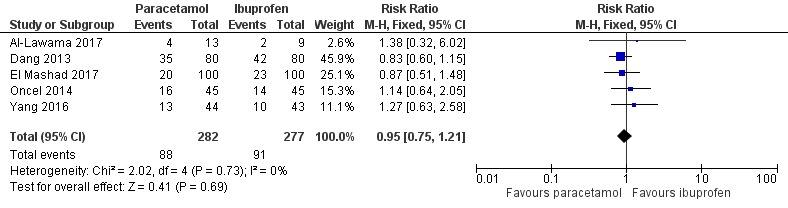
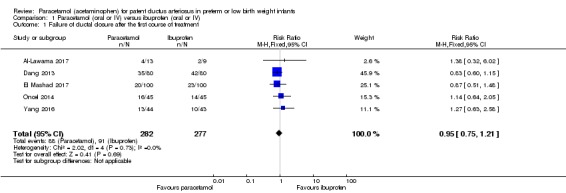
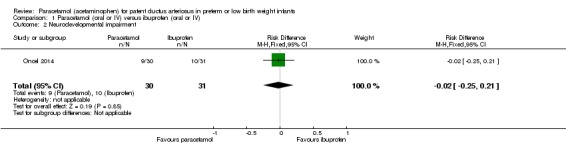
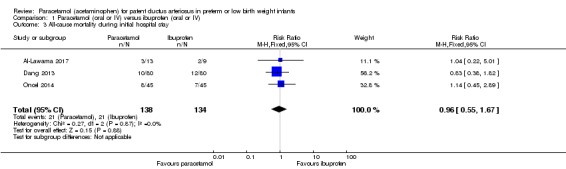
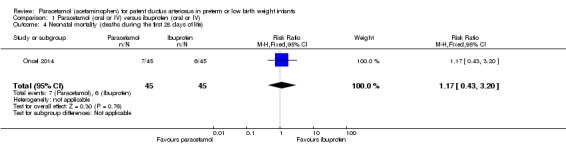
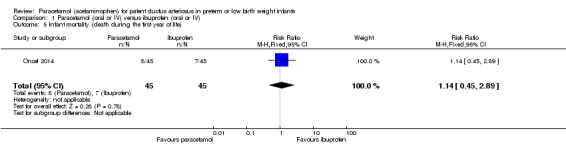
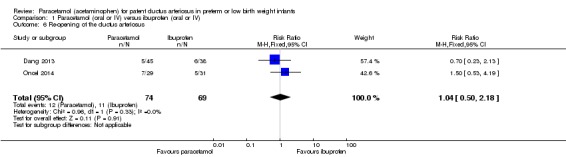
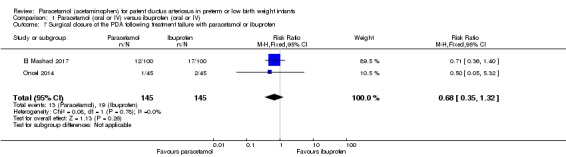
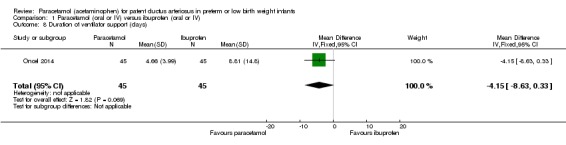
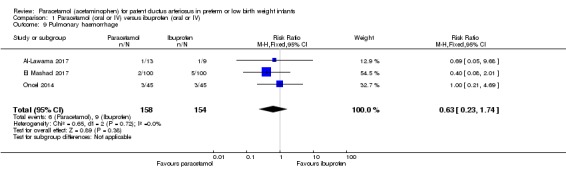
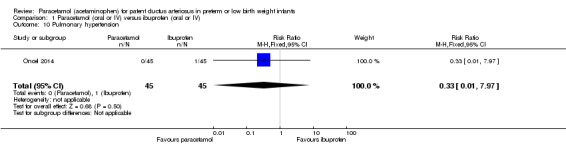
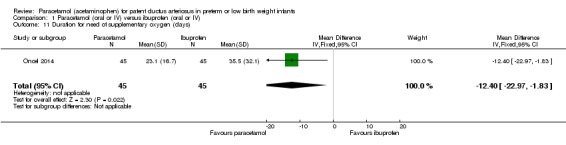
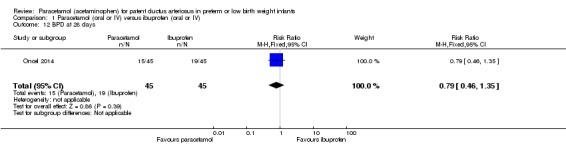
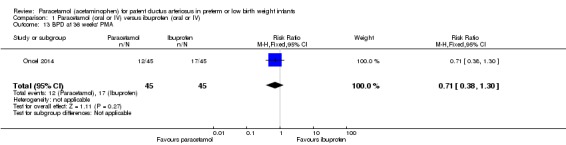
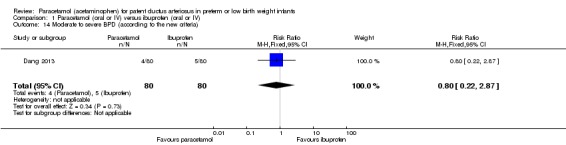
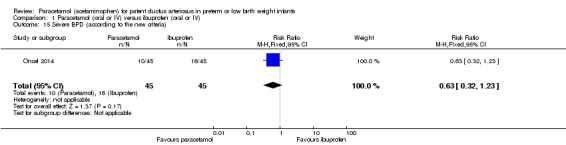
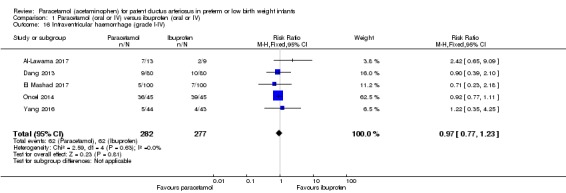
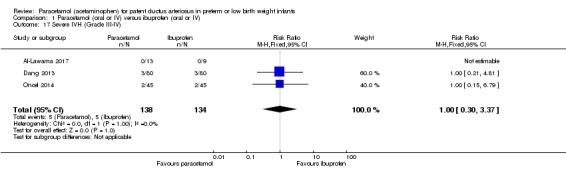
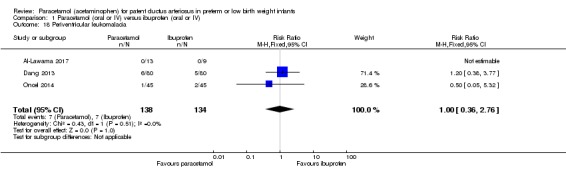
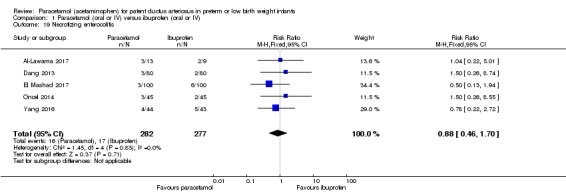
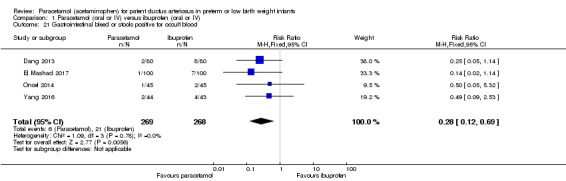
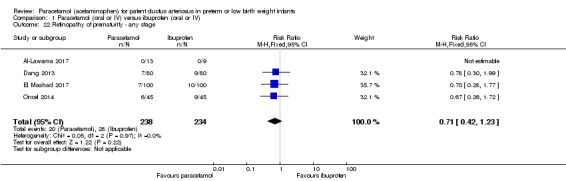
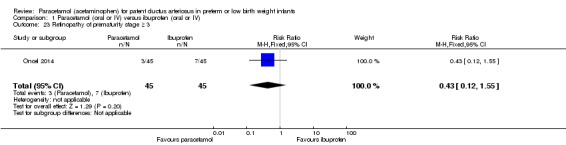
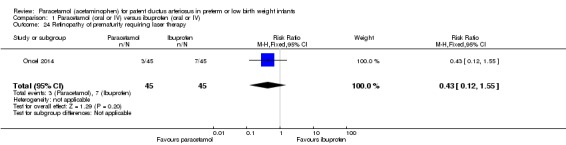
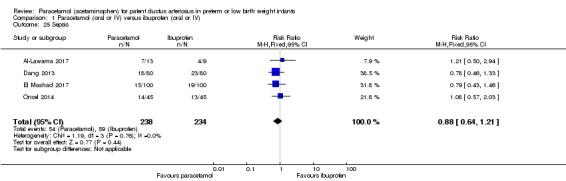
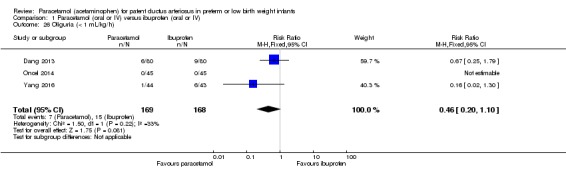
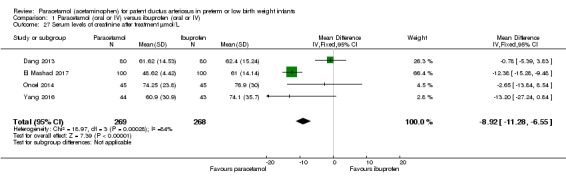
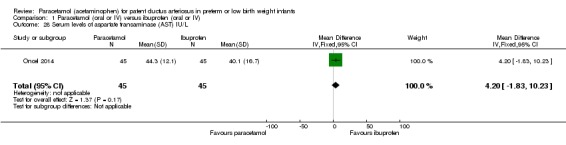
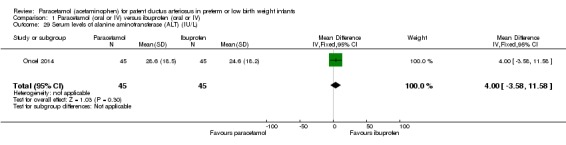
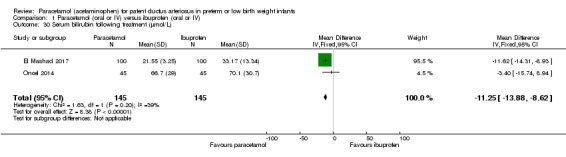
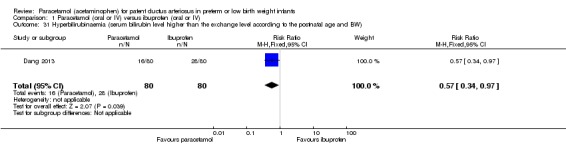
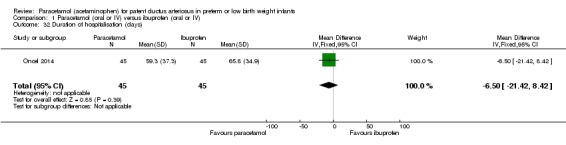
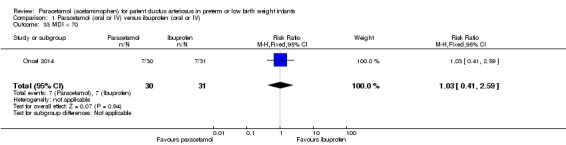
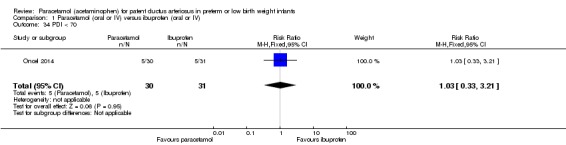
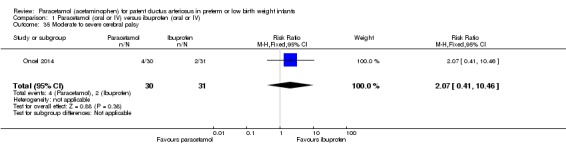
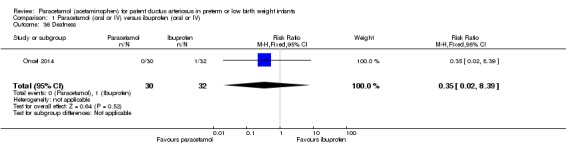
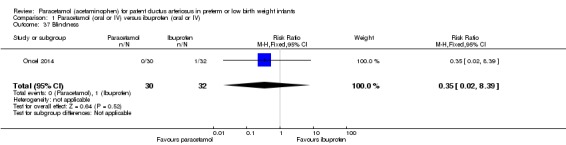
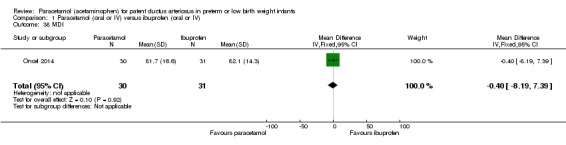
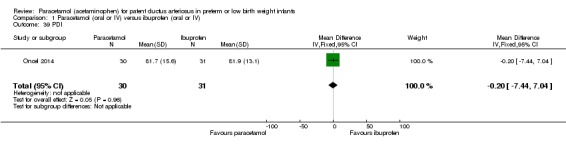
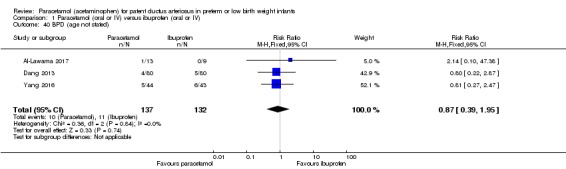
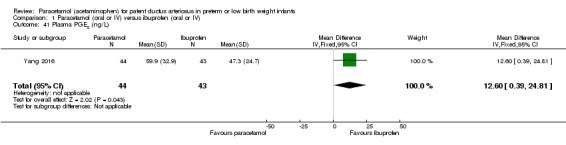
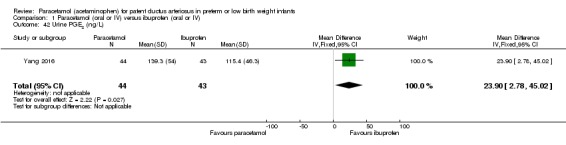
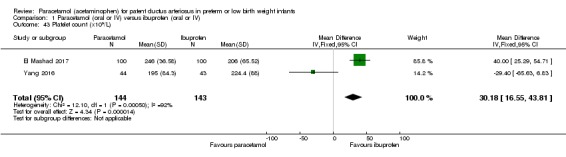
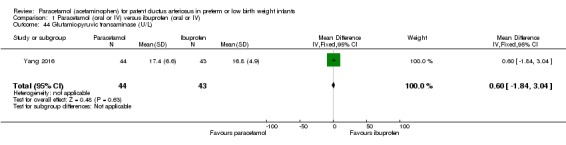
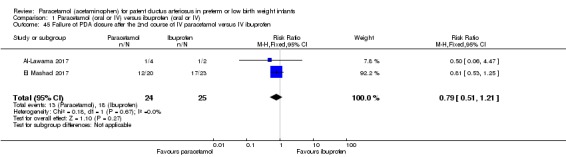
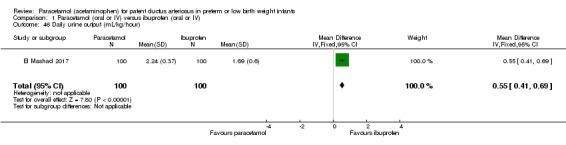
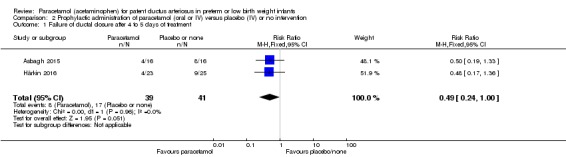
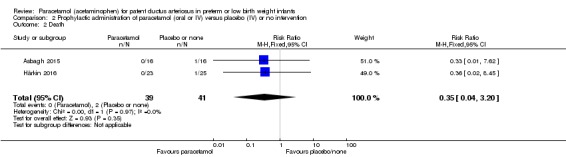
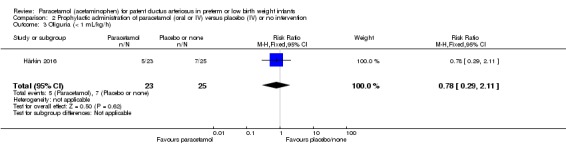
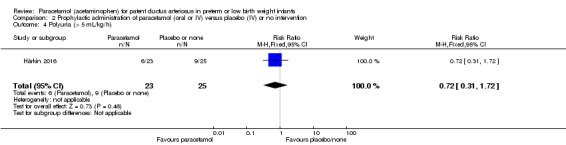
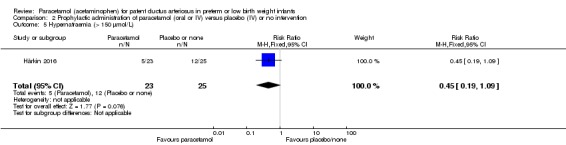
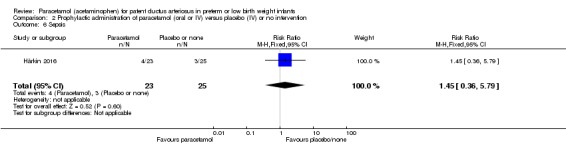
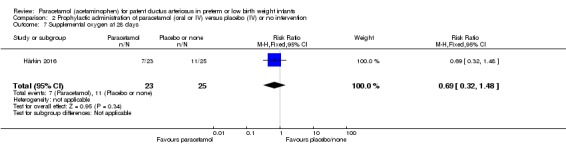
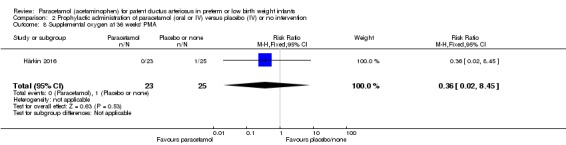
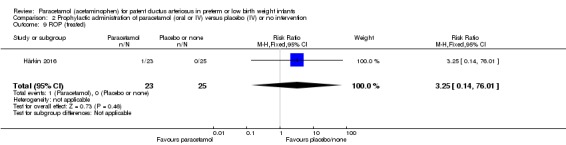
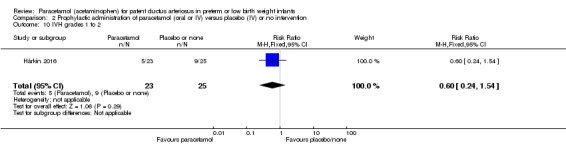
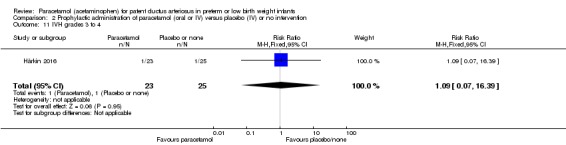
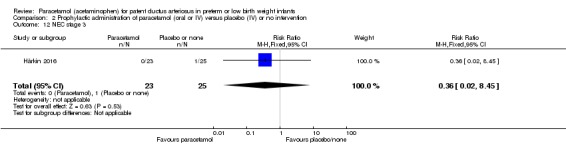
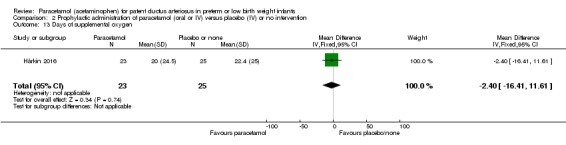
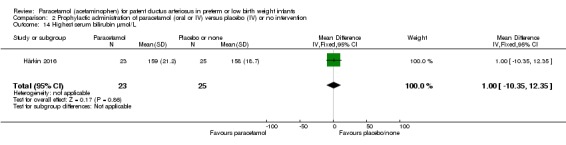
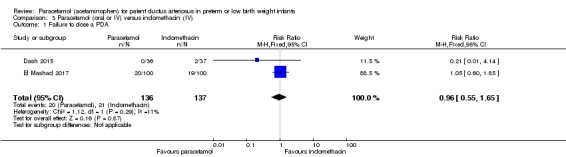
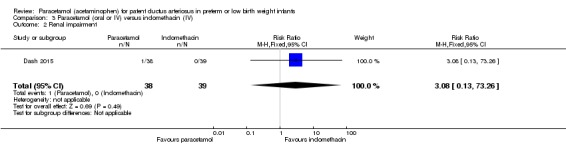
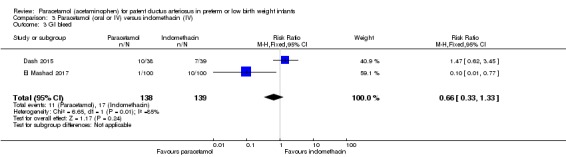
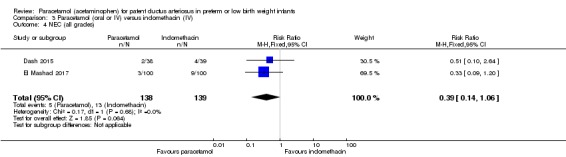
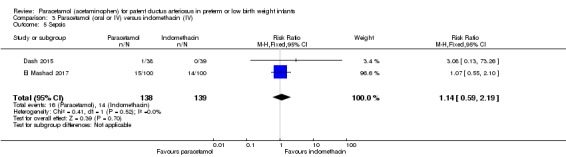
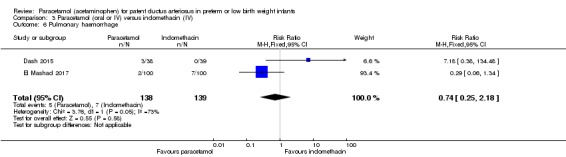
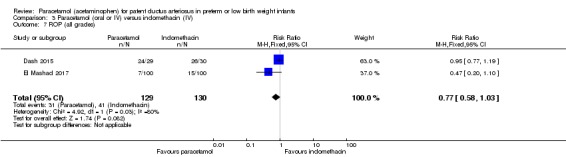
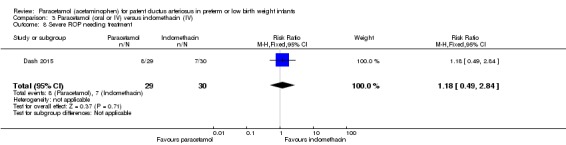
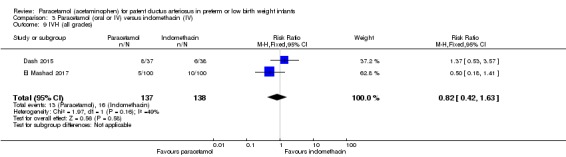
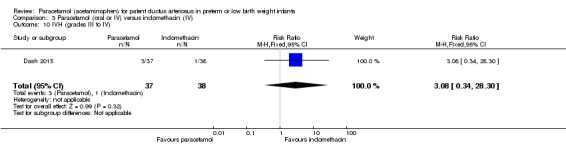
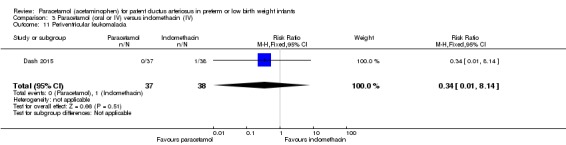
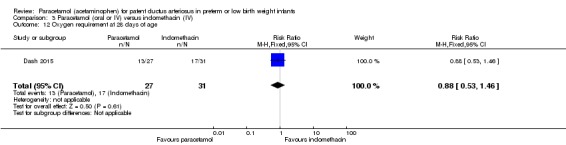
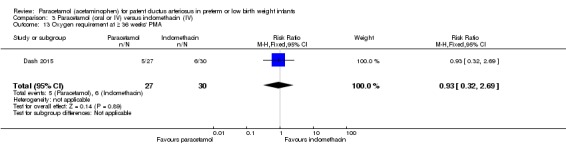
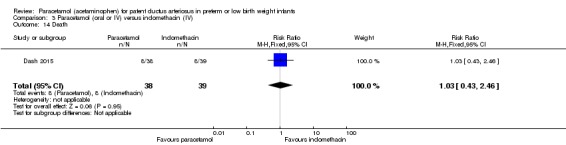
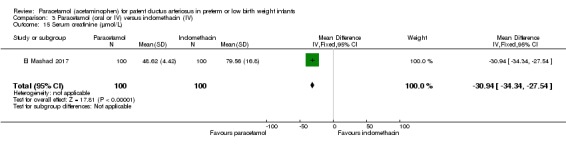
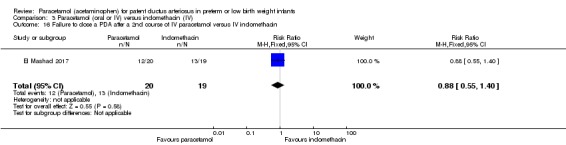
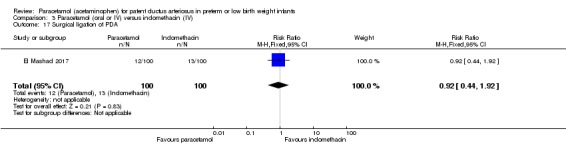
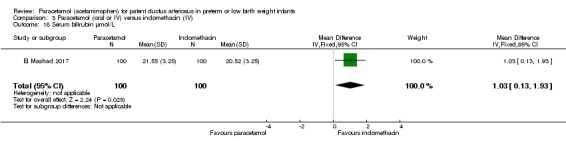
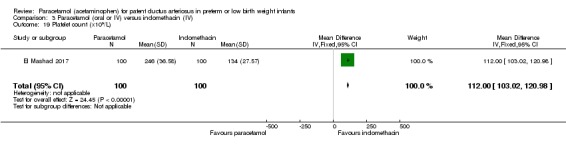
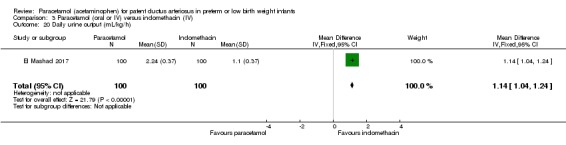
Main results: We included eight studies that reported on 916 infants. One of these studies compared paracetamol to both ibuprofen and indomethacin. Five studies compared treatment of PDA with paracetamol versus ibuprofen and enrolled 559 infants. There was no significant difference between paracetamol and ibuprofen for failure of ductal closure after the first course of drug administration (typical risk ratio (RR) 0.95, 95% confidence interval (CI) 0.75 to 1.21; typical risk difference (RD) -0.02, 95% CI -0.09 to 0.09); I² = 0% for RR and RD; moderate quality of evidence. Four studies (n = 537) reported on gastrointestinal bleed which was lower in the paracetamol group versus the ibuprofen group (typical RR 0.28, 95% CI 0.12 to 0.69; typical RD -0.06, 95% CI -0.09 to -0.02); I² = 0% for RR and RD; number needed to treat for an additional beneficial outcome (NNTB) 17 (95% CI 11 to 50); moderate quality of evidence. The serum levels of creatinine were lower in the paracetamol group compared with the ibuprofen group in four studies (moderate quality of evidence), as were serum bilirubin levels following treatment in two studies (n = 290). Platelet counts and daily urine output were higher in the paracetamol group compared with the ibuprofen group. One study reported on long-term follow-up to 18 to 24 months of age following treatment with paracetamol versus ibuprofen. There were no significant differences in the neurological outcomes at 18 to 24 months (n = 61); (low quality of evidence).Two studies compared prophylactic administration of paracetamol for a PDA with placebo or no intervention in 80 infants. Paracetamol resulted in a lower rate of failure of ductal closure after 4 to 5 days of treatment compared to placebo or no intervention which was of borderline significance for typical RR 0.49 (95% CI 0.24 to 1.00; P = 0.05); but significant for typical RD -0.21 (95% CI -0.41 to -0.02); I² = 0 % for RR and RD; NNTB 5 (95% CI 2 to 50); (low quality of evidence).Two studies (n = 277) compared paracetamol with indomethacin. There was no significant difference in the failure to close a PDA (typical RR 0.96, 95% CI 0.55 to 1.65; I² = 11%; typical RD -0.01, 95% CI -0.09 to 0.08; I² = 17%) (low quality of evidence). Serum creatinine levels were significantly lower in the paracetamol group compared with the indomethacin group and platelet counts and daily urine output were significantly higher in the paracetamol group.
Authors' conclusions: Moderate-quality evidence according to GRADE suggests that paracetamol is as effective as ibuprofen; low-quality evidence suggests paracetamol to be more effective than placebo or no intervention; and low-quality evidence suggests paracetamol as effective as indomethacin in closing a PDA. There was no difference in neurodevelopmental outcome in children exposed to paracetamol compared to ibuprofen; however the quality of evidence is low and comes from only one study. In view of concerns raised regarding neurodevelopmental outcomes following prenatal and postnatal exposure to paracetamol, long-term follow-up to at least 18 to 24 months' postnatal age must be incorporated in any studies of paracetamol in the newborn population. At least 19 ongoing trials have been registered. Such trials are required before any recommendations for the possible routine use of paracetamol in the newborn population can be made.
Conflict of interest statement
Arne Ohlsson ‒ no conflict of interest to declare.
Prakeshkumar Shah ‒ no conflict of interest to declare.
Figures
Update of
-
Paracetamol (acetaminophen) for patent ductus arteriosus in preterm or low-birth-weight infants.Cochrane Database Syst Rev. 2015 Mar 11;(3):CD010061. doi: 10.1002/14651858.CD010061.pub2. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2018 Apr 06;4:CD010061. doi: 10.1002/14651858.CD010061.pub3. PMID: 25758061 Updated.
References
References to studies included in this review
-
- Asbagh PA, Zarkesh MR, Nili F, Sadat Nayeri FS, Naeem AT. Prophylactic treatment with oral paracetamol for patent ductus arteriosus in preterm infants: a randomized clinical trial. Tehran University Medical Journal 2015;73(2):86‐92. [http://tumj.tums.ac.ir/article‐1‐6603‐en.html]
-
- Dash SK, Kabra NS, Avasthi BS, Sharma SR, Padhi P, Ahmed J. Enteral paracetamol or intravenous indomethacin for closure of patent ductus arteriosus in preterm neonates: a randomized controlled trial. Indian Pediatrics 2015;52(7):573‐8. [PUBMED: 26244949] - PubMed
- Kabra NS, Dash SK. Comparison of enteral paracetamol and intravenous indomethacin in closure of patent ductus arteriosus (PDA) in preterm newborns: A randomized controlled trial. Pediatric Academic Societies Annual Meeting; 2014 07 17‐18; Vienna, Austria. 2014.
-
- El‐Mashad AE, El‐Mahdy H, Amrousy DE, Elgendy M. Comparative study of the efficacy and safety of paracetamol, ibuprofen, and indomethacin in closure of patent ductus arteriosus in preterm neonates. European Journal of Pediatrics 2017;176(2):233‐40. [DOI: 10.1007/s00431-016-2830-7; PUBMED: 28004188] - DOI - PubMed
References to studies awaiting assessment
-
- Babaei H, Nemati R, Daryoshi H. Closure of patent ductus arteriosus with oral acetaminophen in preterm neonates: A randomized trial. Biomedical Research and Therapy 2018;5(2):2034‐44.
-
- Kluckow MR, Carlisle H, Broom M, Woods P, Jeffery M, Desai D, et al. A randomised blinded placebo controlled trial of paracetamol to treat later PDA. Journal of Paediatrics and Child Health 2016;52(Suppl 2):100.
References to ongoing studies
-
- ACTRN12613000289718. Paracetamol for patent ductus arteriosus treatment: comparison between oral and intravenous administration. Australian New Zealand Clinical Trials Registry (first received 8 March 2013).
-
- ACTRN12616001517460. Early paracetamol (EPAR) to promote early closure of the ductus arteriosus in preterm infants. Australian New Zealand Clinical Trials Registry (first received 1 November 2016).
-
- CTRI/2016/09/007261. Oral ibuprofen versus paracetamol on ductus arteriosus [Comparison of oral paracetamol versus ibuprofen for PDA closure in preterms ‐ a randomized controlled single blinded study ‐ IPOD]. apps.who.int/trialsearch/Trial2.aspx?TrialID=CTRI/2016/09/007261 (first received 8 September 2016).
-
- CTRI/2017/10/009989. Paracetamol versus ibuprofen for closure of patent ductus arteriosus [Efficacy and safety of oral paracetamol versus oral ibuprofen in management of patent ductus arteriosus in preterm neonates less than or equal to 34 Weeks or less than or equal to 1800 gms: a randomized control trial ‐ BAP trial]. apps.who.int/trialsearch/Trial2.aspx?TrialID=CTRI/2017/10/009989 (first received 10 October 2017).
Additional references
-
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th Edition. Arlington, VA: American Psychiatric Association, 2013.
-
- Arana A, Morton NS, Hansen TG. Treatment with paracetamol in infants. Acta Anaesthesiologica Scandinavica 2001;45(1):20‐9. [PUBMED: 11152028] - PubMed
-
- Avella‐Garcia CB, Julvez J, Fortuny J, Rebordosa C, García‐Esteban R, Galán IR, et al. Acetaminophen use in pregnancy and neurodevelopment: attention function and autism spectrum symptoms. International Journal of Epidemiology 2016;45(6):1987‐96. [DOI: 10.1093/ije/dyw115; PUBMED: 27353198] - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous