

Analysis of prognostic factors for survival in patients with primary spinal chordoma using the SEER Registry from 1973 to 2014
- PMID: 29625617
- PMCID: PMC5889560
- DOI: 10.1186/s13018-018-0784-3
Analysis of prognostic factors for survival in patients with primary spinal chordoma using the SEER Registry from 1973 to 2014
Abstract
Background: Spinal chordomas are rare primary osseous tumors that arise from the remnants of the notochord. They are commonly considered slow-growing, locally invasive neoplasms with little tendency to metastasize, but the high recurrent rate of spinal chordomas may seriously affect the survival rate and quality of life of patients. The aim of the study is to describe the epidemiological data and determine the prognostic factors for decreased survival in patients with primary spinal chordoma.
Methods: The Surveillance, Epidemiology, and End Results (SEER) Registry database, a US population-based cancer registry database, was used to identify all patients diagnosed with primary spinal chordoma from 1973 to 2014. We utilized Kaplan-Meier method and Cox proportional hazards regression analysis to evaluate the association between patients overall survival and relevant characteristics, including age, gender, race, disease stage, treatment methods, primary tumor site, marital status, and urban county background.
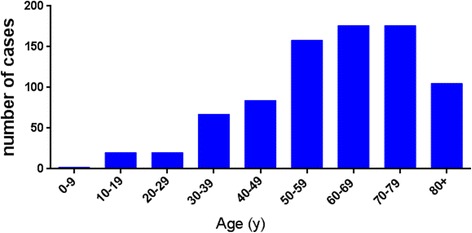
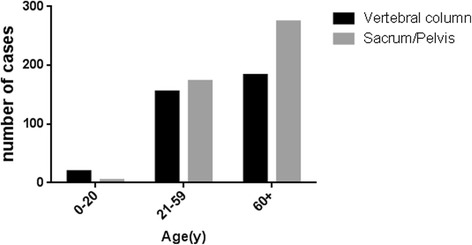
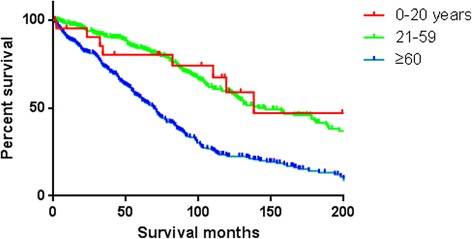
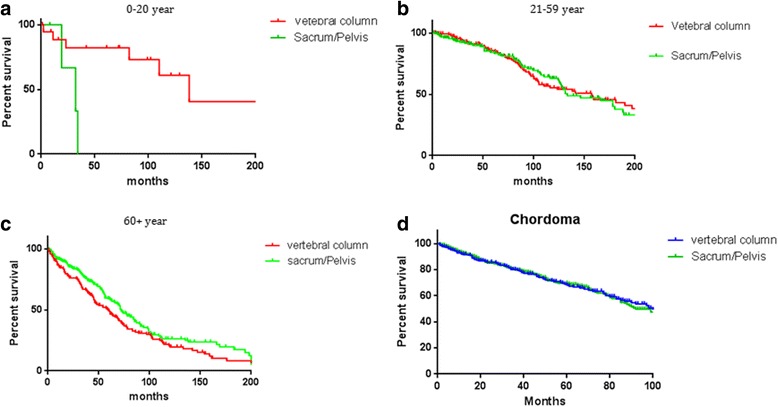
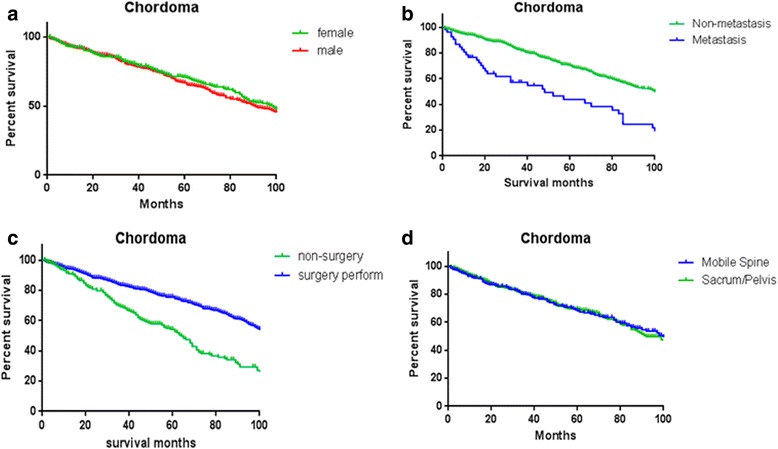
Results: In the data set between 1973 and 2014, a total of 808 patients were identified with primary spinal chordoma. The overall rate of distant metastatic cases in our cohort was only 7.7%. Spinal chordoma was more common occurred in men (62.6%) than women (37.3%). Majority of neoplasms were found in the White (87.9%), while the incidence of the Black is relatively infrequent (3.3%). Three hundred fifty-seven spinal chordomas (44.2%) were located in the vertebral column, while 451 patients' tumor (55.8%) was located in the sacrum or pelvis. Age ≥ 60 years (HR = 2.72; 95%CI, 1.71 to 2.89), distant metastasis (HR = 2.16; 95%CI, 1.54 to 3.02), and non-surgical therapy (HR = 2.14; 95%CI, 1.72 to 2.69) were independent risk factors for survival reduction in analysis. Survival did not significantly differ as a factor of tumor site (vertebrae vs sacrum/pelvis) for primary spinal chordoma (HR = 0.93, P = 0.16). Race (P = 0.52), gender (P = 0.11), marital status (P = 0.94), and urban background (P = 0.72) were not main factors which affected overall survival rate.
Conclusion: There was no significant difference in overall survival rate between chordomas located in the sacrum and vertebral column. Spinal chordoma patients with an elderly age (age ≥ 60), performing non-surgical therapy, and distant metastasis were associated with worse overall survival. Performing surgery was an effective and reliable treatment method for patients with spinal chordoma, and public health efforts should pay more attention to the elderly patients with spinal chordoma prior to distant metastasis.
Keywords: Osseous neoplasm; Prognostic factors; SEER; Spinal chordoma.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
