

Acute encephalitis - diagnosis and management
- PMID: 29626021
- PMCID: PMC6303463
- DOI: 10.7861/clinmedicine.18-2-155
Acute encephalitis - diagnosis and management
Abstract
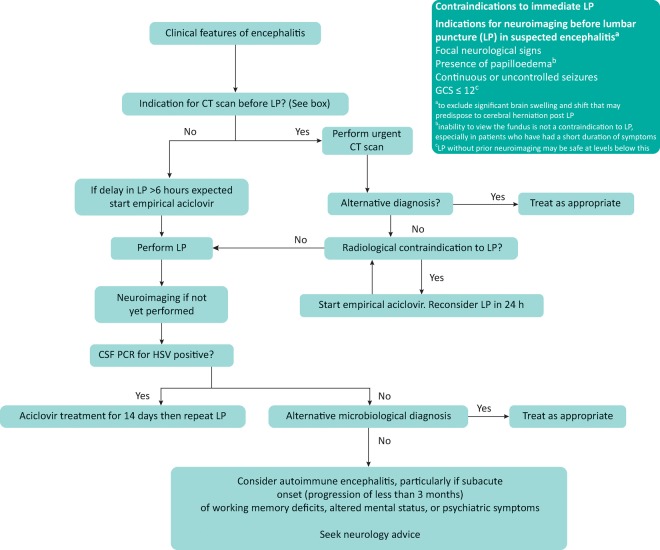
Encephalitis, inflammation of the brain, is most commonly caused by a viral infection (especially herpes simplex virus [HSV] type 1 in the UK) although autoimmune causes, such as N-methyl D-aspartate receptor (NMDAR) antibody encephalitis, are increasingly recognised. Most patients present with a change in consciousness level and may have fever, seizures, movement disorder or focal neurological deficits. Diagnosis hinges crucially on lumbar puncture and cerebrospinal fluid (CSF) examination, but imaging and electroencephalography (EEG) may also be helpful. Treatment of HSV encephalitis with aciclovir dramatically improves outcome, but the optimal management of autoimmune encephalitis is still uncertain. Many patients with encephalitis are left with residual physical or neuropsychological deficits which require long-term multidisciplinary management. Here we review assessment of patients with suspected encephalitis, general aspects of management and areas of ongoing research.
Keywords: brain infection; confusion; encephalitis; encephalopathy; lumbar puncture.
© Royal College of Physicians 2018. All rights reserved.
Figures
Comment in
-
Comment on CME Infectious diseases.Clin Med (Lond). 2018 Jun;18(3):269. doi: 10.7861/clinmedicine.18-3-269. Clin Med (Lond). 2018. PMID: 29858448 Free PMC article. No abstract available.
-
Response.Clin Med (Lond). 2018 Jun;18(3):269-270. doi: 10.7861/clinmedicine.18-3-269a. Clin Med (Lond). 2018. PMID: 29858449 Free PMC article. No abstract available.
References
-
- Michael B. Menezes BF. Cunniffe J, et al. Effect of delayed lumbar punctures on the diagnosis of acute bacterial meningitis in adults. Emerg Med J. 2010;27:433–8. - PubMed
-
- Granerod J. Ambrose HE. Davies NW, et al. Causes of encephalitis and differences in their clinical presentations in England: a multicentre, population-based prospective study. Lancet Infect Dis. 2010;10:835–44. - PubMed
-
- Glaser CA. Gilliam S. Schnurr D, et al. In search of encephalitis etiologies: diagnostic challenges in the California Encephalitis Project, 1998–2000. Clin Infect Dis. 2003;36:731–42. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
