

Metabolomic Profiling in Acute ST-Segment-Elevation Myocardial Infarction Identifies Succinate as an Early Marker of Human Ischemia-Reperfusion Injury
- PMID: 29626151
- PMCID: PMC6015393
- DOI: 10.1161/JAHA.117.007546
Metabolomic Profiling in Acute ST-Segment-Elevation Myocardial Infarction Identifies Succinate as an Early Marker of Human Ischemia-Reperfusion Injury
Abstract
Background: Ischemia-reperfusion injury following ST-segment-elevation myocardial infarction (STEMI) is a leading determinant of clinical outcome. In experimental models of myocardial ischemia, succinate accumulation leading to mitochondrial dysfunction is a major cause of ischemia-reperfusion injury; however, the potential importance and specificity of myocardial succinate accumulation in human STEMI is unknown. We sought to identify the metabolites released from the heart in patients undergoing primary percutaneous coronary intervention for emergency treatment of STEMI.
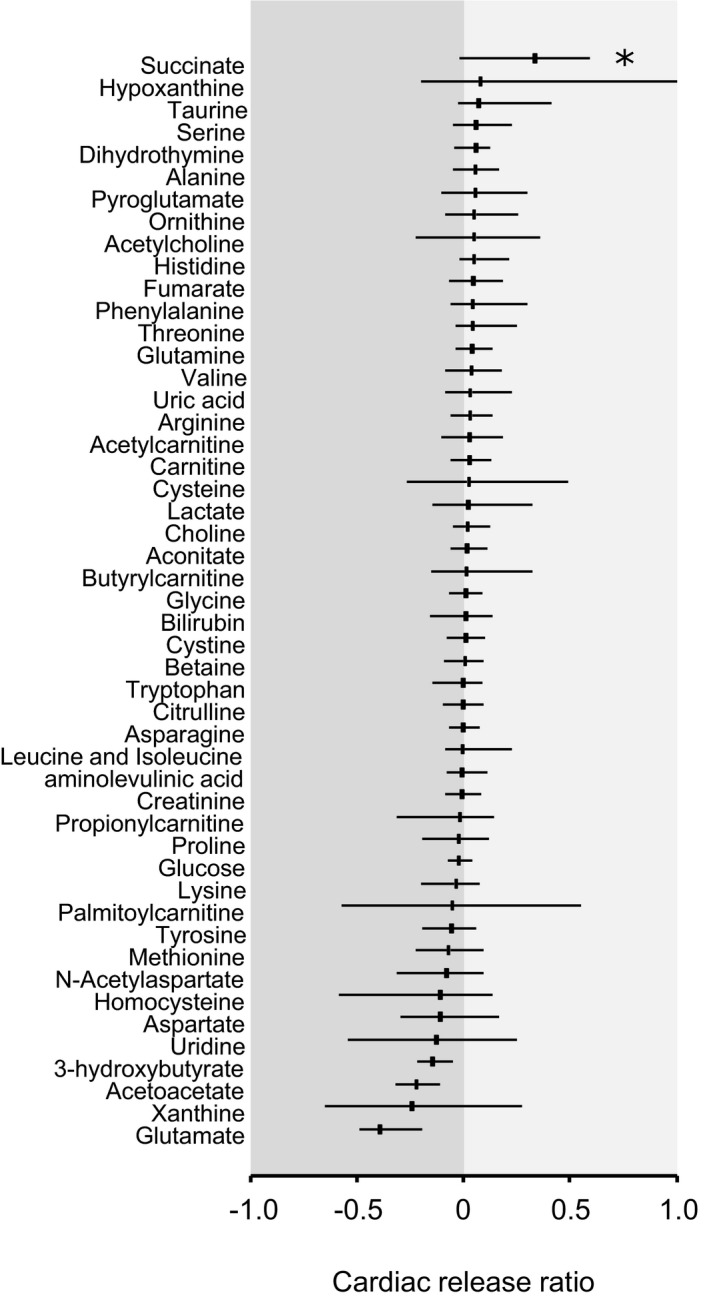
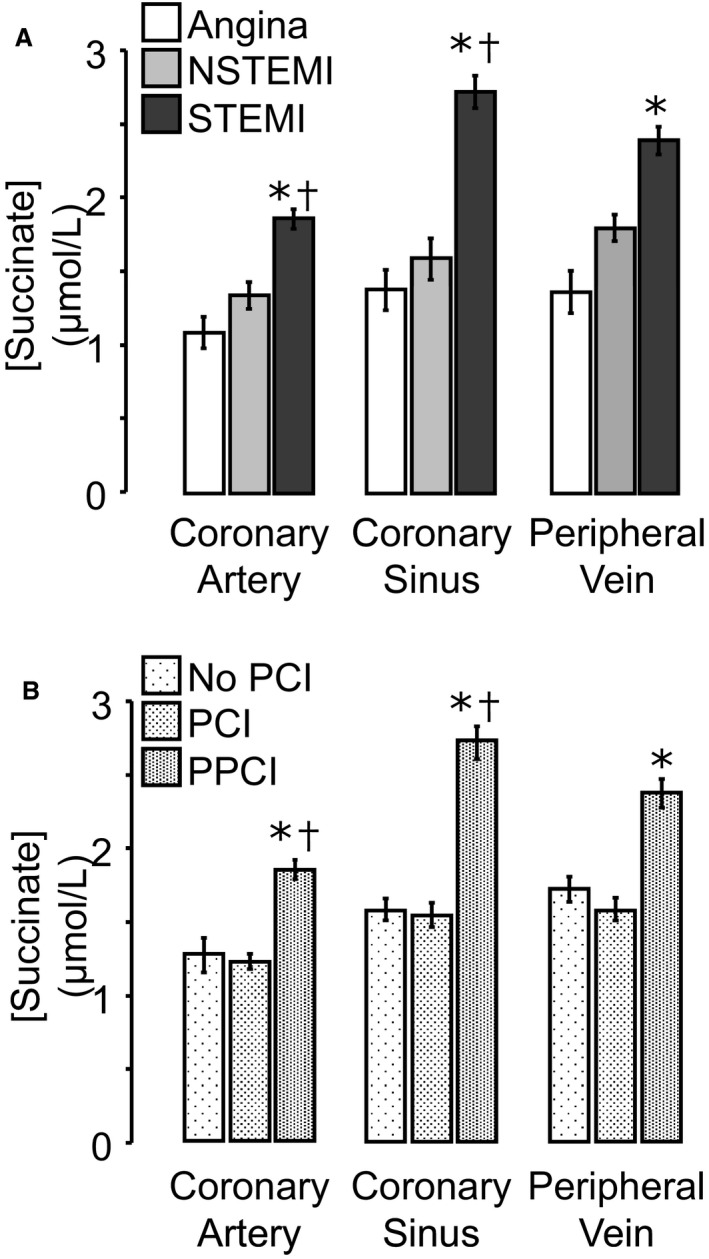
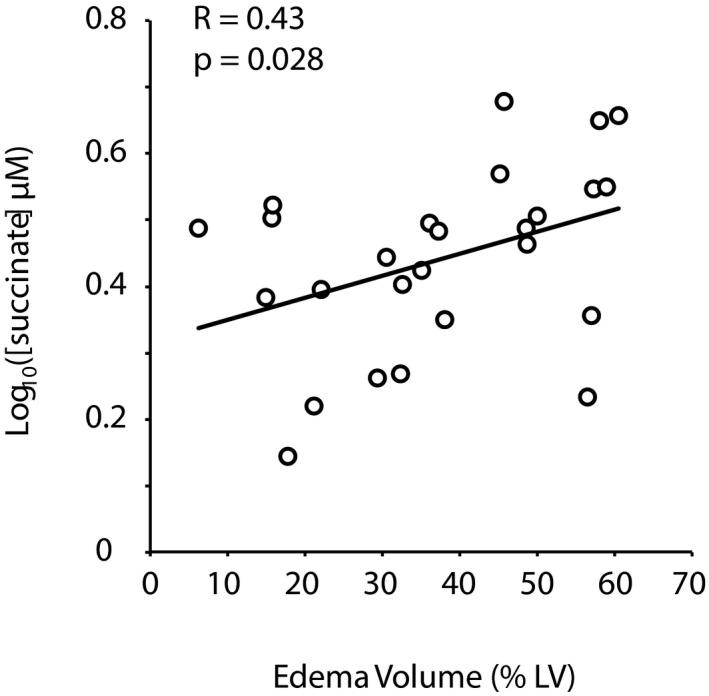
Methods and results: Blood samples were obtained from the coronary artery, coronary sinus, and peripheral vein in patients undergoing primary percutaneous coronary intervention for acute STEMI and in control patients undergoing nonemergency coronary angiography or percutaneous coronary intervention for stable angina or non-STEMI. Plasma metabolites were analyzed by targeted liquid chromatography and mass spectrometry. Metabolite levels for coronary artery, coronary sinus, and peripheral vein were compared to derive cardiac and systemic release ratios. In STEMI patients, cardiac magnetic resonance imaging was performed 2 days and 6 months after primary percutaneous coronary intervention to quantify acute myocardial edema and final infarct size, respectively. In total, 115 patients undergoing acute STEMI and 26 control patients were included. Succinate was the only metabolite significantly increased in coronary sinus blood compared with venous blood in STEMI patients, indicating cardiac release of succinate. STEMI patients had higher succinate concentrations in arterial, coronary sinus, and peripheral venous blood than patients with non-STEMI or stable angina. Furthermore, cardiac succinate release in STEMI correlated with the extent of acute myocardial injury, quantified by cardiac magnetic resonance imaging.
Conclusion: Succinate release by the myocardium correlates with the extent of ischemia.
Keywords: ischemia–reperfusion injury; mitochondria; myocardial ischemia; myocardial metabolism.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Cung T‐T, Morel O, Cayla G, Rioufol G, Garcia‐Dorado D, Angoulvant D, Bonnefoy‐Cudraz E, Guérin P, Elbaz M, Delarche N, Coste P, Vanzetto G, Metge M, Aupetit J‐F, Jouve B, Motreff P, Tron C, Labeque J‐N, Steg PG, Cottin Y, Range G, Clerc J, Claeys MJ, Coussement P, Prunier F, Moulin F, Roth O, Belle L, Dubois P, Barragan P, Gilard M, Piot C, Colin P, De Poli F, Morice M‐C, Ider O, Dubois‐Randé J‐L, Unterseeh T, Le Breton H, Béard T, Blanchard D, Grollier G, Malquarti V, Staat P, Sudre A, Elmer E, Hansson MJ, Bergerot C, Boussaha I, Jossan C, Derumeaux G, Mewton N, Ovize M. Cyclosporine before PCI in patients with acute myocardial infarction. N Engl J Med. 2015;373:1021–1031. - PubMed
-
- Chouchani ET, Pell VR, Gaude E, Aksentijević D, Sundier SY, Robb EL, Logan A, Nadtochiy SM, Ord ENJ, Smith AC, Eyassu F, Shirley R, Hu C‐H, Dare AJ, James AM, Rogatti S, Hartley RC, Eaton S, Costa ASH, Brookes PS, Davidson SM, Duchen MR, Saeb‐Parsy K, Shattock MJ, Robinson AJ, Work LM, Frezza C, Krieg T, Murphy MP. Ischaemic accumulation of succinate controls reperfusion injury through mitochondrial ROS. Nature. 2014;515:431–435. - PMC - PubMed
-
- Lee R, Antonopoulos AS, Alexopoulou Z, Margaritis M, Kharbanda RK, Choudhury RP, Antoniades C, Channon KM. Artifactual elevation of plasma sCD40L by residual platelets in patients with coronary artery disease. Int J Cardiol. 2013;168:1648–1650. - PubMed
-
- Cuculi F, Dall'Armellina E, Manlhiot C, De Caterina AR, Colyer S, Ferreira V, Morovat A, Prendergast BD, Forfar JC, Alp NJ, Choudhury RP, Neubauer S, Channon KM, Banning AP, Kharbanda RK. Early change in invasive measures of microvascular function can predict myocardial recovery following PCI for ST‐elevation myocardial infarction. Eur Heart J. 2014;35:1971–1980. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
