

Advances in predictive in vitro models of drug-induced nephrotoxicity
- PMID: 29626199
- PMCID: PMC6013592
- DOI: 10.1038/s41581-018-0003-9
Advances in predictive in vitro models of drug-induced nephrotoxicity
Abstract
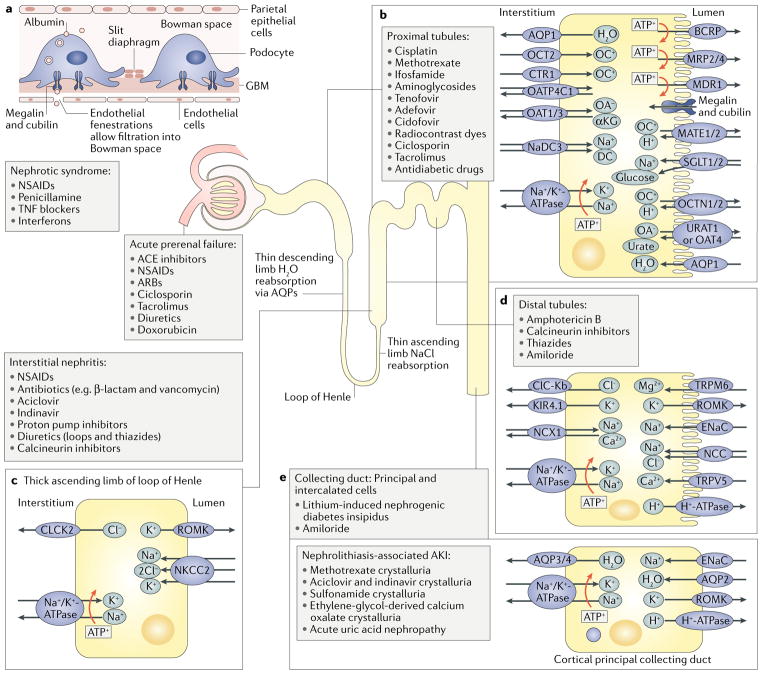
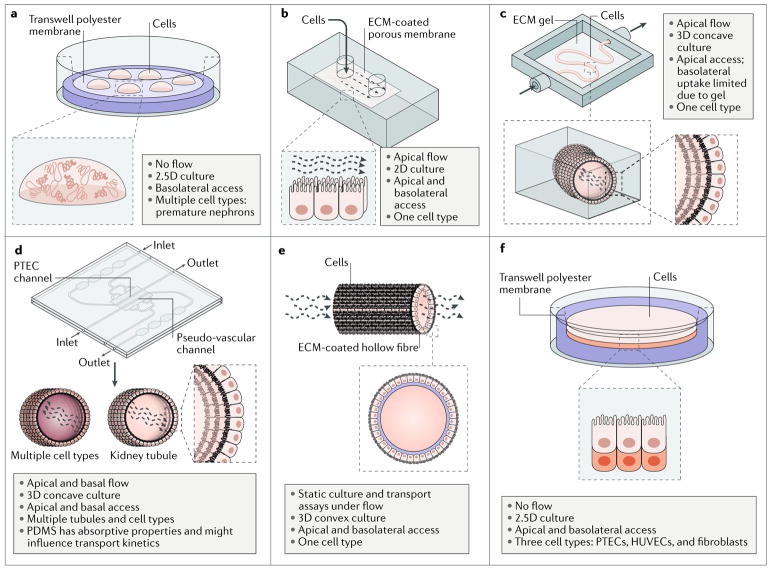
In vitro screens for nephrotoxicity are currently poorly predictive of toxicity in humans. Although the functional proteins that are expressed by nephron tubules and mediate drug susceptibility are well known, current in vitro cellular models poorly replicate both the morphology and the function of kidney tubules and therefore fail to demonstrate injury responses to drugs that would be nephrotoxic in vivo. Advances in protocols to enable the directed differentiation of pluripotent stem cells into multiple renal cell types and the development of microfluidic and 3D culture systems have opened a range of potential new platforms for evaluating drug nephrotoxicity. Many of the new in vitro culture systems have been characterized by the expression and function of transporters, enzymes, and other functional proteins that are expressed by the kidney and have been implicated in drug-induced renal injury. In vitro platforms that express these proteins and exhibit molecular biomarkers that have been used as readouts of injury demonstrate improved functional maturity compared with static 2D cultures and represent an opportunity to model injury to renal cell types that have hitherto received little attention. As nephrotoxicity screening platforms become more physiologically relevant, they will facilitate the development of safer drugs and improved clinical management of nephrotoxicants.
Conflict of interest statement
M.H.L. holds a research contract with Organovo, Inc. The other authors declare no competing interests.
Figures
References
-
- Nolin TD, Himmelfarb J. In: Adverse Drug Reactions. Uetrecht J, editor. Springer; Berlin, Heidelberg: 2010. pp. 111–130.
-
- Grünfeld JP, Rossier BC. Lithium nephrotoxicity revisited. Nat Rev Nephrol. 2009;5:270–276. - PubMed
-
- Rewa O, Bagshaw SM. Acute kidney injury — epidemiology, outcomes and economics. Nat Rev Nephrol. 2014;10:193–207. - PubMed
-
- Magee TV, et al. Discovery of Dap-3 polymyxin analogues for the treatment of multidrug-resistant Gram-negative nosocomial infections. J Med Chem. 2013;56:5079–5093. - PubMed
-
- Tiong HY, et al. Drug-induced nephrotoxicity: clinical impact and preclinical in vitro models. Mol Pharm. 2014;11:1933–1948. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
