

Atrial Fibrillation in the ICU
- PMID: 29627355
- PMCID: PMC6335260
- DOI: 10.1016/j.chest.2018.03.040
Atrial Fibrillation in the ICU
Abstract
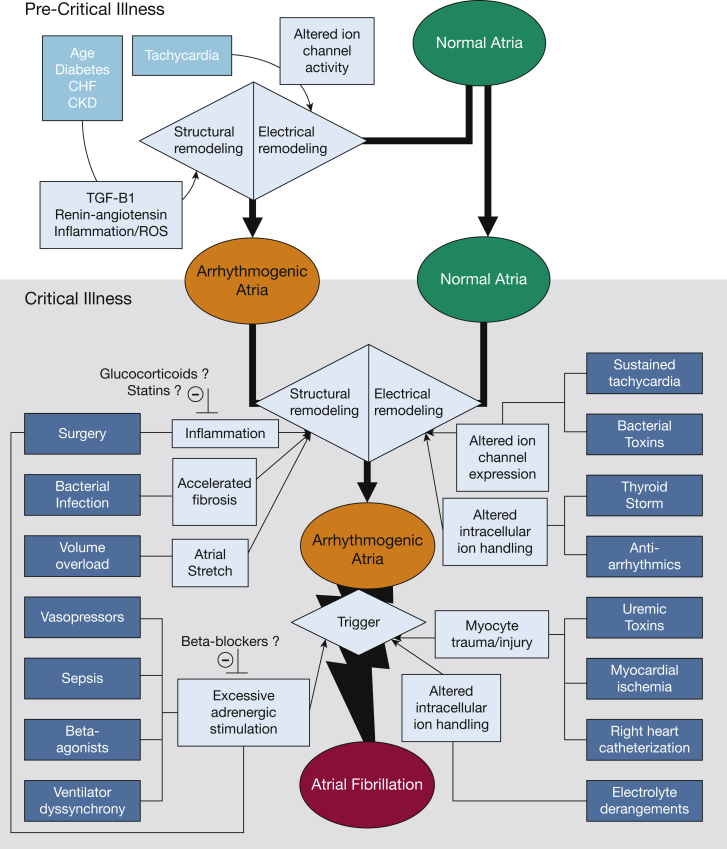
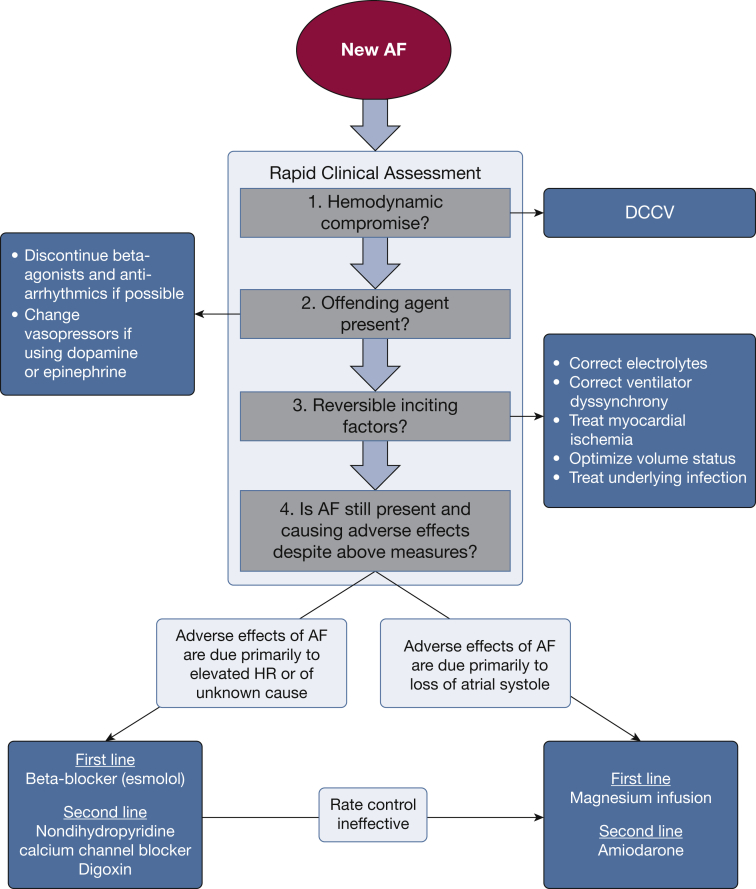
Atrial fibrillation (AF) is the most common arrhythmia encountered in the ICU. Preexisting AF is highly prevalent among older patients with chronic conditions who are at risk for critical illness, whereas new-onset AF can be triggered by accelerated atrial remodeling and arrhythmogenic triggers encountered during critical illness. The acute loss of atrial systole and onset of rapid ventricular rates that characterize new-onset AF often lead to decreased cardiac output and hemodynamic compromise. Thus, new-onset AF is both a marker of disease severity as well as a likely contributor to poor outcomes, similar to other manifestations of organ dysfunction during critical illness. Evaluating immediate hemodynamic effects of new-onset AF during critical illness is an important component of rapid clinical assessment aimed at identifying patients in need of urgent direct current cardioversion, treatment of reversible inciting factors, and identification of patients who may benefit from pharmacologic rate or rhythm control. In addition to acute hemodynamic effects, new-onset AF during critical illness is associated with both short- and long-term increases in the risk of stroke, heart failure, and death, with AF recurrence rates of approximately 50% within 1 year following hospital discharge. In the absence of a strong evidence base, there is substantial practice variation in the choice of strategies for management of new-onset AF during critical illness. We describe acute and long-term evaluation and management strategies based on current evidence and propose future avenues of investigation to fill large knowledge gaps in the management of patients with AF during critical illness.
Keywords: atrial fibrillation; critical illness; sepsis.
Copyright © 2018 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Lloyd-Jones D.M., Wang T.J., Leip E.P. Lifetime risk for development of atrial fibrillation: the Framingham Heart Study. Circulation. 2004;110(9):1042–1046. - PubMed
-
- Benjamin E.J., Wolf P.A., D'Agostino R.B., Silbershatz H., Kannel W.B., Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98(10):946–952. - PubMed
-
- Wolf P.A., Dawber T.R., Thomas H.E., Jr., Kannel W.B. Epidemiologic assessment of chronic atrial fibrillation and risk of stroke: the Framingham study. Neurology. 1978;28(10):973–977. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
