

Syndemics: A theory in search of data or data in search of a theory?
- PMID: 29628175
- PMCID: PMC6613368
- DOI: 10.1016/j.socscimed.2018.03.040
Syndemics: A theory in search of data or data in search of a theory?
Abstract
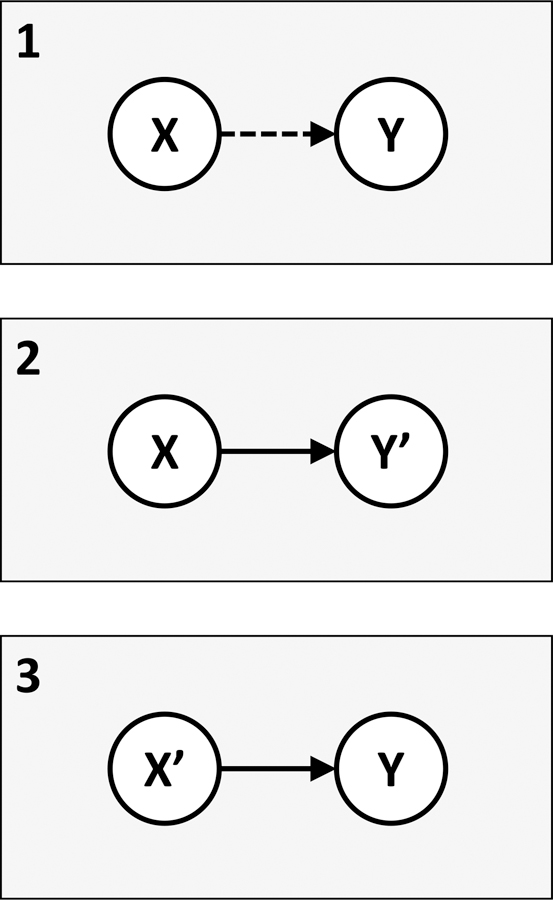
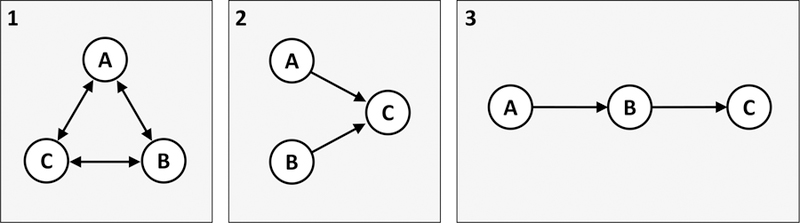
The concept of a syndemic was proposed more than two decades ago to explain how large-scale social forces might give rise to co-occurring epidemics that synergistically interact to undermine health in vulnerable populations. This conceptual instrument has the potential to help policymakers and program implementers in their endeavors to improve population health. Accordingly, it has become an increasingly popular heuristic for advocacy, most notably in the field of HIV treatment and prevention. However, most empirical studies purporting to validate the theory of syndemics actually do no such thing. Tomori et al. (2018) provide a novel case study from India illustrating how the dominant empirical approach fails to promote deeper understanding about how hazardous alcohol use, illicit drug use, depression, childhood sexual abuse, and intimate partner violence interact to worsen HIV risk among men who have sex with men. In this commentary, I relate the theory of syndemics to other established social science and public health theories of disease distribution, identify possible sources of conceptual and empirical confusion, and provide concrete suggestions for how to validate the theory using a mixed-methods approach. The hope is that more evidence can be mobilized -- whether informed by the theory of syndemics or not -- to improve health and psychosocial wellbeing among vulnerable populations worldwide.
Keywords: HIV; Mixed methods; Multilevel analysis; Population health; Social determinants of health; Stigma; Syndemic; Syndemics.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Figures
References
-
- Adeboye A, Ross MW, Wilkerson MJ, Springer A, Ahaneku H, Yusuf RA, et al. (2017). Syndemic production of HIV infection among Tanzanian MSM. Journal of Health Education Research & Development, 5(3), 1000231.
-
- Agar M (2005). Agents in living color: towards emic agent-based models. Journal of Artificial Societies and Social Simulation, 8(1).
-
- Bearman PS, Moody J, & Stovel K (2004). Chains of affection: the structure of adolescent romantic and sexual networks. American Journal of Sociolology, 110(1), 44–91.
-
- Bekhuis E, Schoevers RA, van Borkulo CD, Rosmalen JG, & Boschloo L (2016). The network structure of major depressive disorder, generalized anxiety disorder and somatic symptomatology. Psychological Medicine, 46(14), 2989–2998. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
