

Permanent Deployment of the Solitaire FR™ Device in the Basilar Artery in an Acute Stroke Scenario
- PMID: 29628939
- PMCID: PMC5881145
- DOI: 10.1159/000480245
Permanent Deployment of the Solitaire FR™ Device in the Basilar Artery in an Acute Stroke Scenario
Abstract
Background: Scarce reports exist of permanent deployment of Solitaire FR™ devices for arterial steno-occlusive disease as it is primarily indicated for temporary deployment for thrombectomy in large-vessel, anterior-circulation ischemic strokes. Even more scarce are reports describing permanent deployment of the Solitaire device for posterior circulation strokes.
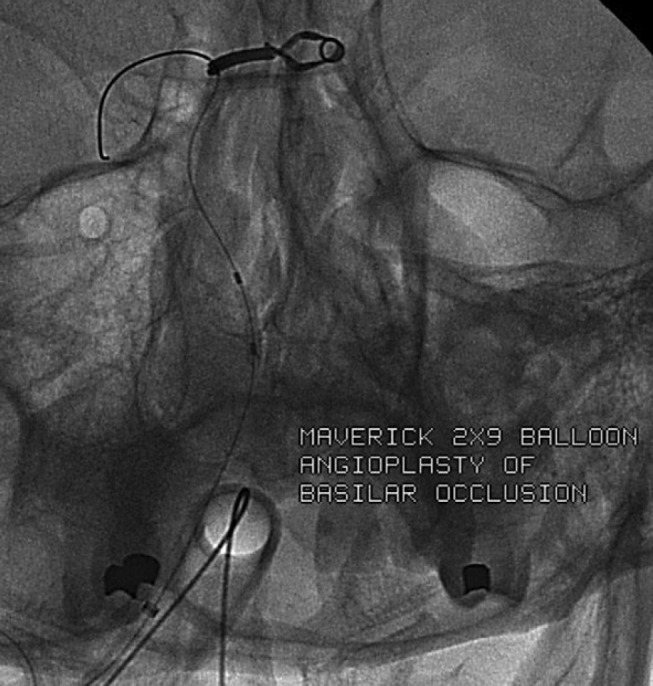
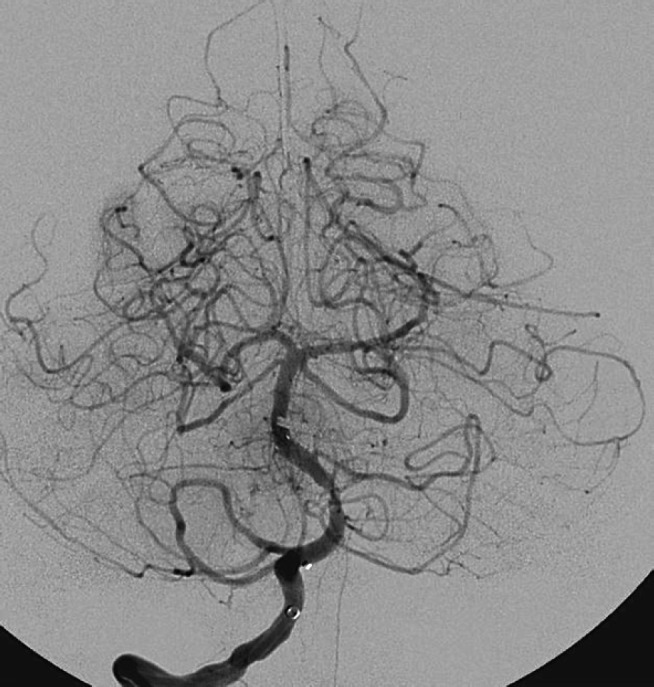
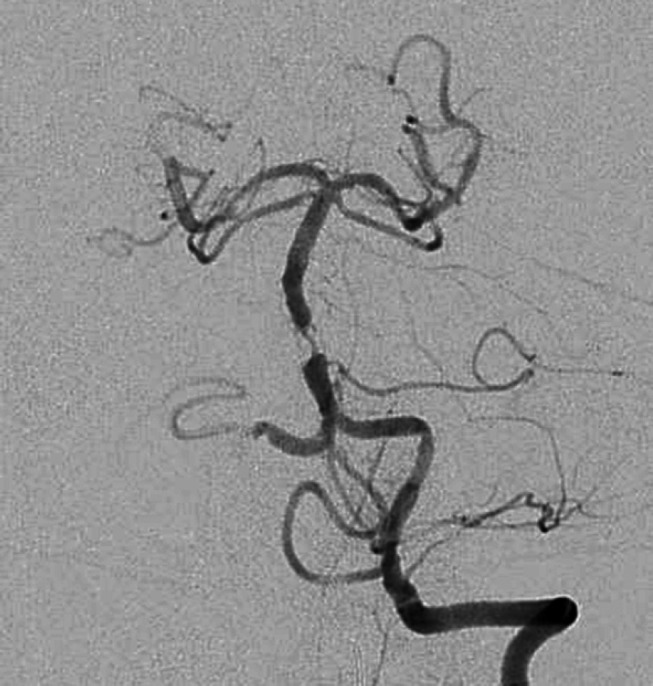
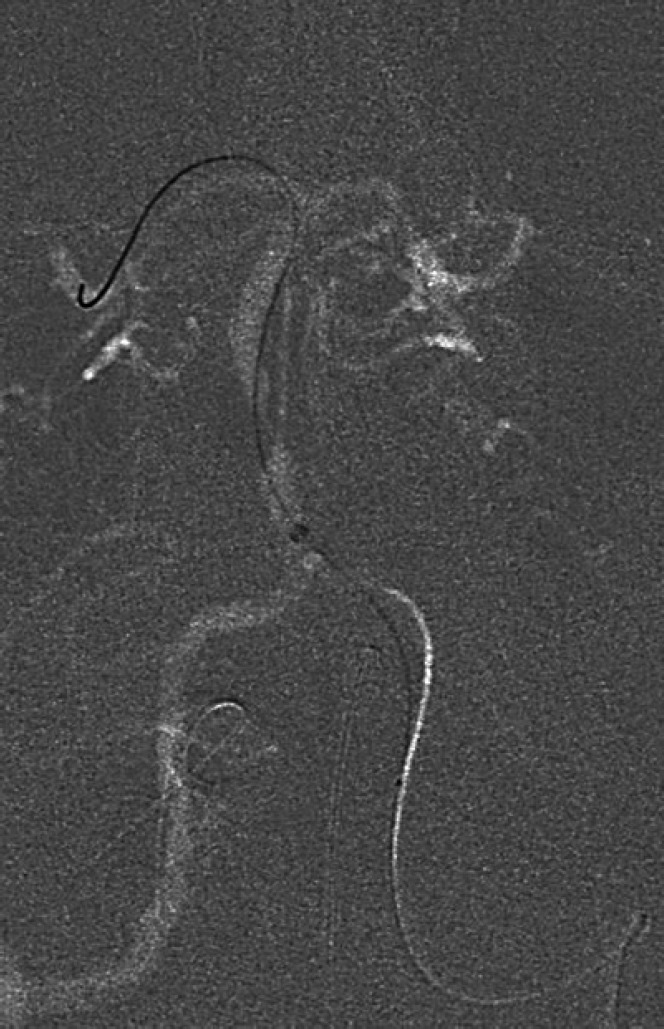
Summary: We present 2 cases where the Solitaire device was electrolytically detached to re-establish flow in an occluded or stenotic basilar artery in acutely symptomatic patients. In both cases, a 4 × 15 mm Solitaire device was positioned across the stenotic or occluded portion of the basilar artery and electrolytically detached to maintain vessel patency. Both cases had good clinical outcomes with a National Institutes of Health Stroke Scale (NIHSS) score of 1 (from 24) on 90-day follow-up and an NIHSS score of 2 (from 7) on 30-day follow-up.
Key messages: Permanent deployment of the Solitaire device may potentially be a safe and effective means of maintaining vessel patency in an occluded or stenotic basilar artery.
Keywords: Acute stroke; Solitaire; Thrombectomy.
Figures




References
-
- Berkhemer OA, Puck SS, Fransen MD, Beumer D, van den Berg LA, Lingsma HF, et al. MR CLEAN Investigators A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372:11–20. - PubMed
-
- Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornon J, et al. ESCAPE Trial Investigators Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 2015;372:1019–1030. - PubMed
-
- Campbell BCV, Mitchell PJ, Kleinig TJ, Dewey HM, Churiloy L, Yassi N, et al. EXTEND-IA Investigators Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015;372:1009–1018. - PubMed
-
- Saver JL, Goyal M, Diener HC, Levy EI, Pereira VM, et al. SWIFT PRIME Investigators Stent-retriever thrombectomy after intravenous t-PA versus t-PA alone in stroke. N Engl J Med. 2015;372:2285–2295. - PubMed
-
- Jovin TG, Chamorro A, Cobo E, de Miquel M, Molina CA, Rovira A, et al. REVASCAT Trial Investigators Thrombectomy within 8 h after symptom onset in ischemic stroke. N Engl J Med. 2015;372:2296–2306. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
