

Endoscopy-assisted craniosynostosis surgery followed by helmet therapy
- PMID: 29629226
- PMCID: PMC5875112
- DOI: 10.4103/sni.sni_17_18
Endoscopy-assisted craniosynostosis surgery followed by helmet therapy
Abstract
Background: Surgical methods to treat craniosynostosis have evolved from a simple strip craniectomy to a diverse spectrum of partial or complete cranial vault remodeling with excellent results but often with high comorbidity. Therefore, minimal invasive craniosynostosis surgery has been explored in the last few decades. The main goal of minimal invasive craniosynostosis surgery is to reduce the morbidity and invasiveness of classical surgical procedures, with equal long-term results, both functional as well as cosmetic.
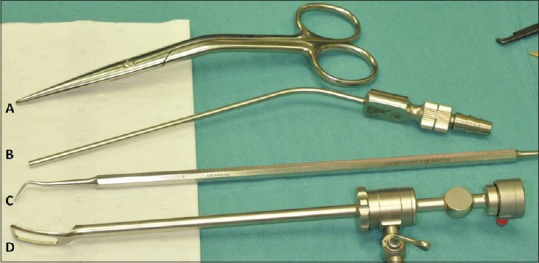
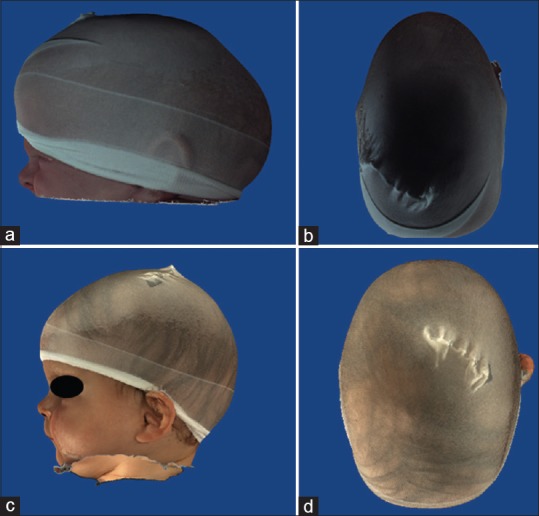
Methods: To reach these goals, we adopted endoscopy-assisted craniosynostosis surgery (EACS) supplemented with helmet molding therapy in 2005.
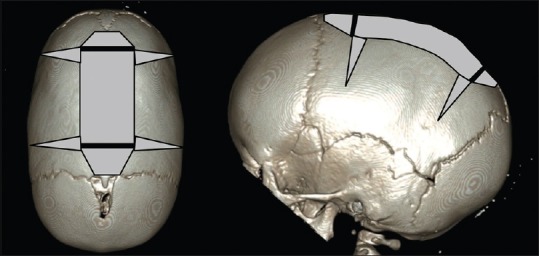
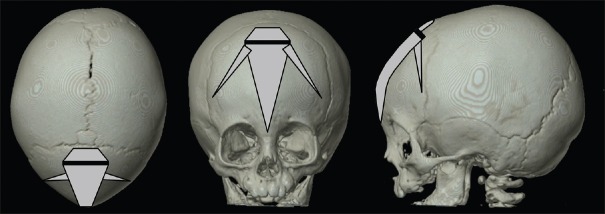
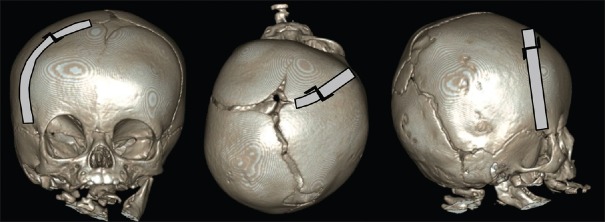
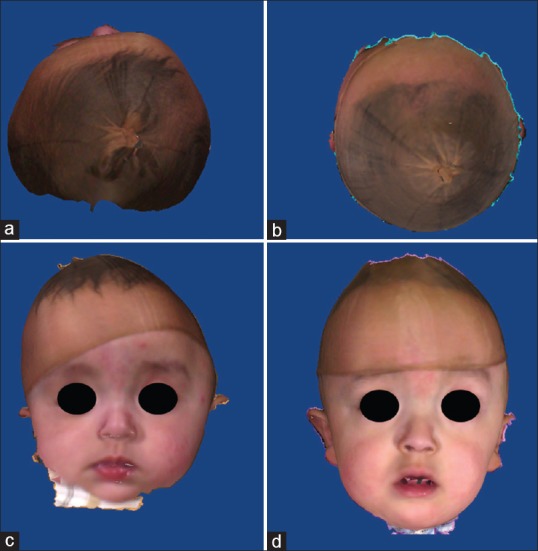
Results: We present in detail our surgical technique used for scaphocephaly, trigonocephaly, plagiocephaly, complex multisutural, and syndromic cases of craniosynostosis.
Conclusions: We conclude that EACS with helmet therapy is a safe and suitable treatment option for any type of craniosynostosis, if performed at an early age, preferably around 3 months of age.
Keywords: Craniosynostosis; endoscopy; helmet; minimal invasive; surgical technique.
Conflict of interest statement
None of the authors have any conflict of interest with publication of the manuscript or an institution or product that is mentioned in the manuscript and/or is important to the outcome of the study presented.
Figures


References
-
- Anderson FM, Johnson FL. Craniosynostosis; a modification in surgical treatment. Surgery. 1956;40:961–70. - PubMed
-
- Arnaud E, Marchac A, Jeblaoui Y, Renier D, Di Rocco F. Spring-assisted posterior skull expansion without osteotomies. Childs Nerv Syst. 2012;28:1545–9. - PubMed
-
- Berry-Candelario J, Ridgway EB, Grondin RT, Rogers GF, Proctor MR. Endoscope-assisted strip craniectomy and postoperative helmet therapy for treatment of craniosynostosis. Neurosurg Focus. 2011;31:E5. - PubMed
-
- Chan JW, Stewart CL, Stalder MW, St. Hilaire H, McBride L, Moses MH. Endoscope-assisted versus open repair of craniosynostosis: A comparison of perioperative cost and risk. J Craniofac Surg. 2013;24:170–4. - PubMed
-
- Delashaw JB, Persing JA, Broaddus WC, Jane JA. Cranial vault growth in craniosynostosis. J Neurosurg. 1989;70:159–65. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources