

Atypical Presentation of Pneumocystis jirovecii Infection in HIV Infected Patients: Three Different Manifestations
- PMID: 29629518
- PMCID: PMC5890084
- DOI: 10.3346/jkms.2018.33.e115
Atypical Presentation of Pneumocystis jirovecii Infection in HIV Infected Patients: Three Different Manifestations
Abstract
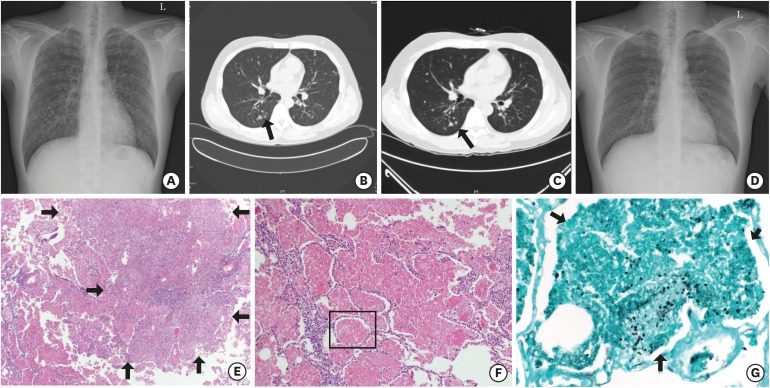
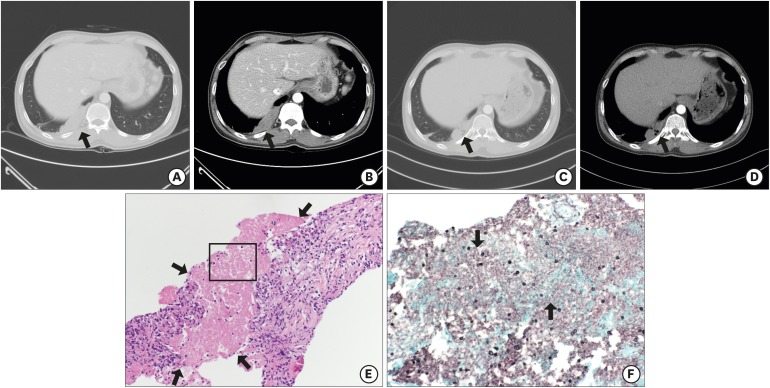
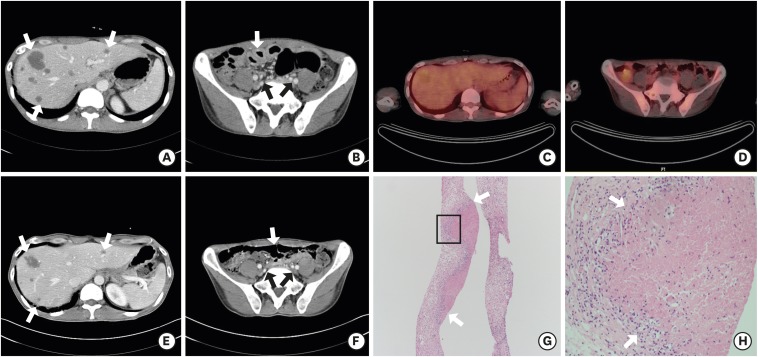
Advances in the treatment and prevention of Pneumocystis jirovecii infection (PJI) in human immunodeficiency virus (HIV) patients decreased incidence and mortality dramatically, however, it may be associated with an increased frequency of unusual manifestation such as cystic formation, pneumothorax, focal infiltration, nodular formation, or extrapulmonary lesions. We report three cases of PJI with atypical manifestations. Each case demonstrates different clinical features: multiple nodular pulmonary lesion (32-year-old man with abnormal chest X-ray finding), subpleural mass-like lesion (43-year-old man with left visual loss and right pleuritic chest pain), and extrapulmonary mass-like lesions in the liver, lymph nodes, and small bowel (39-year-old man with cough, sputum, and dyspnea). P. jirovecii was confirmed in all 3 cases and they were treated well. It is necessary to understand that PJI shows variable clinical features.
Keywords: AIDS; Atypical; Extrapulmonary; HIV; Nodular; Pneumocystis jirovecii.
© 2018 The Korean Academy of Medical Sciences.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Furrer H, Egger M, Opravil M, Bernasconi E, Hirschel B, Battegay M, et al. Discontinuation of primary prophylaxis against Pneumocystis carinii pneumonia in HIV-1 infected adults treated with combination antiretroviral therapy. Swiss HIV Cohort Study. N Engl J Med. 1999;340(17):1301–1306. - PubMed
-
- Kim JM, Cho GJ, Hong SK, Chang KH, Chung JS, Choi YH, et al. Epidemiology and clinical features of HIV infection/AIDS in Korea. Yonsei Med J. 2003;44(3):363–370. - PubMed
-
- Boiselle PM, Crans CA, Jr, Kaplan MA. The changing face of Pneumocystis carinii pneumonia in AIDS patients. AJR Am J Roentgenol. 1999;172(5):1301–1309. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
