

Use of raloxifene and tamoxifen by breast cancer risk level in a Medicare-eligible cohort
- PMID: 29630889
- PMCID: PMC5970073
- DOI: 10.1016/j.ajog.2018.03.031
Use of raloxifene and tamoxifen by breast cancer risk level in a Medicare-eligible cohort
Abstract
Background: Raloxifene and tamoxifen are Food and Drug Administration-approved for breast cancer risk reduction; in 2013, the US Preventive Services Task Force recommended these drugs for breast cancer risk reduction in high-risk women. Information on the use of raloxifene and tamoxifen for breast cancer risk reduction in the general population indicates that the risk is believed to be low; however, there is little literature.
Objective: The purpose of this study was to assess the use of breast cancer risk reduction medications by breast cancer risk level in an older cohort of women.
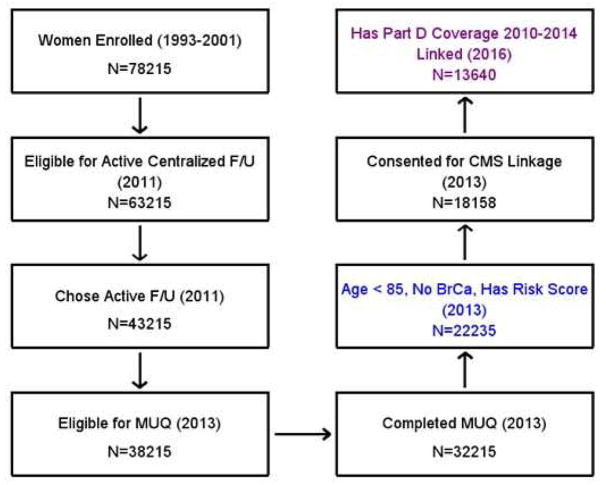
Study design: Women who were enrolled in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial were assessed for the use of raloxifene, tamoxifen, and other medications. The data sources for use of the drugs were a mailed medication use questionnaire in 2013 and linked Medicare Part D claims files from 2010-2014. Estimated breast cancer risk within 5 years was assessed with the use of the modified Gail model and self-reported breast cancer risk factors; comorbidities were assessed through a questionnaire.
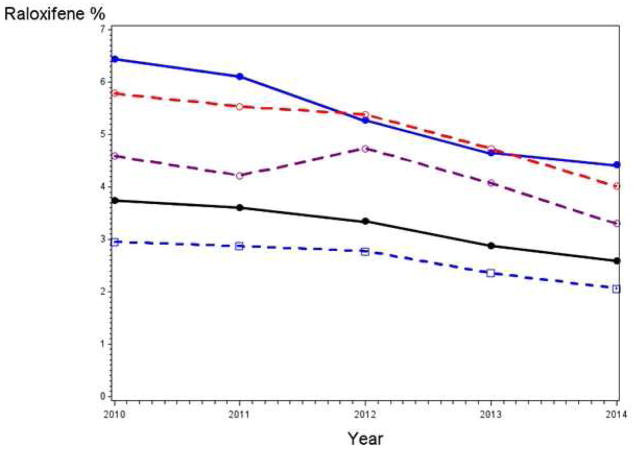
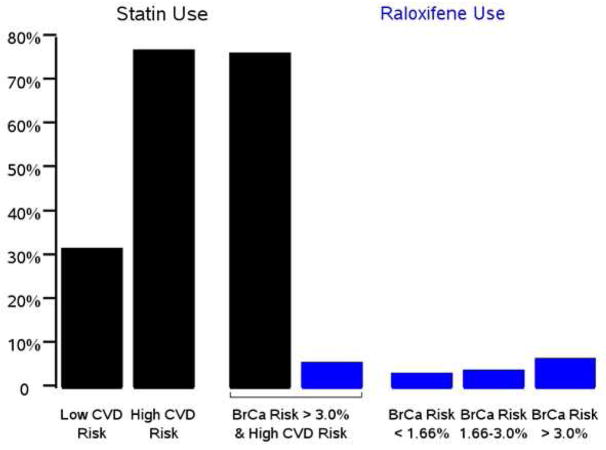
Results: A total of 22,235 women completed the medication use questionnaire; of these, 13,640 women (61%) had linked Part D data. In 2013, 45% of the women were 65-74 years old, and 55% of the women were 75-84 years old. From the medication use questionnaire, raloxifene use (past month) was 1.8%, 2.5%, and 4.0% for women with breast cancer risk within 5 years of <1.66%, 1.66-3.0%, and ≥3%, respectively (probability value trend, <.0001). From Part D, for any use during the period among women with coverage, raloxifene rates were 3.3%, 4.0%, and 6.6% for the 3 categories for breast cancer risk within 5 years (probability value trend, <.0001); use was 7.4% and 3.3% in women with and without osteoporosis, respectively. Raloxifene use significantly decreased from 2010-2014, and specifically from 2012-2014, both for all women and for women with breast cancer risk within 5 years of ≥3%. Tamoxifen use from Part D was 0.36%, 0.45%, and 0.85% for the 3 categories for breast cancer risk within 5 years (probability value trend, .009).
Conclusion: Raloxifene use was low overall but increased modestly with breast cancer risk, and usage decreased from 2010-2014. Tamoxifen use was very low.
Keywords: breast cancer; chemoprevention; raloxifene; risk; tamoxifen.
Published by Elsevier Inc.
Conflict of interest statement
The authors have no conflicts of interest to declare
Figures
References
-
- Fisher B, Constantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 study. J Natl Ca Inst. 1998;90:1371–1388. - PubMed
-
- Vogel VG, Constantino JP, Wickerham DL, et al. Effects of tamoxifen vs raloxifene on the risk of developing invasive breast cancer and other disease outcomes. JAMA. 2006;23:2727–2741. - PubMed
-
- Cauley JA, Norton L, Lippman ME, et al. Continued breast cancer risk reduction in post411 menopausal women treated with raloxifene: 4-year results from the MORE trial. Breast Cancer Res Treat. 2001;65:125–134. - PubMed
-
- Cancer.Gov. [Accessed Oct 2nd, 2017];FDA approval for raloxifene hydrochloride. https://www.cancer.gov/aboutcancer/treatment/drugs/fda-raloxifene-hydroc....
-
- U.S. Department of Health and Human Services, HHS News. [Accessed Oct 2nd, 2017];Tamoxifen approved for reducing breast cancer incidence. http://www3.scienceblog.com/community/older/archives/M/2/fda1168.htm.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
