

Disruption of Renal Arginine Metabolism Promotes Kidney Injury in Hepatorenal Syndrome in Mice
- PMID: 29631342
- PMCID: PMC6173643
- DOI: 10.1002/hep.29915
Disruption of Renal Arginine Metabolism Promotes Kidney Injury in Hepatorenal Syndrome in Mice
Abstract
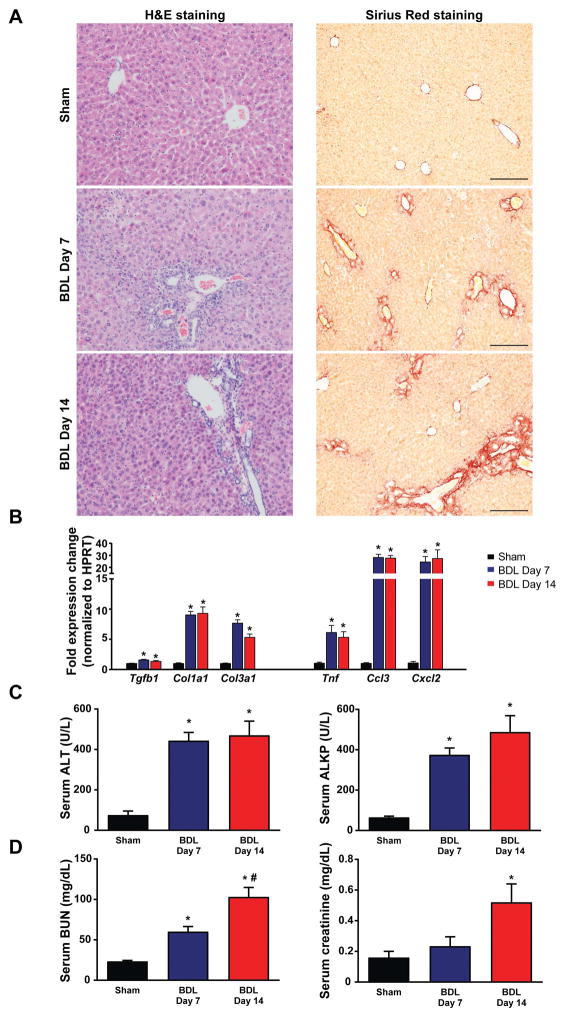
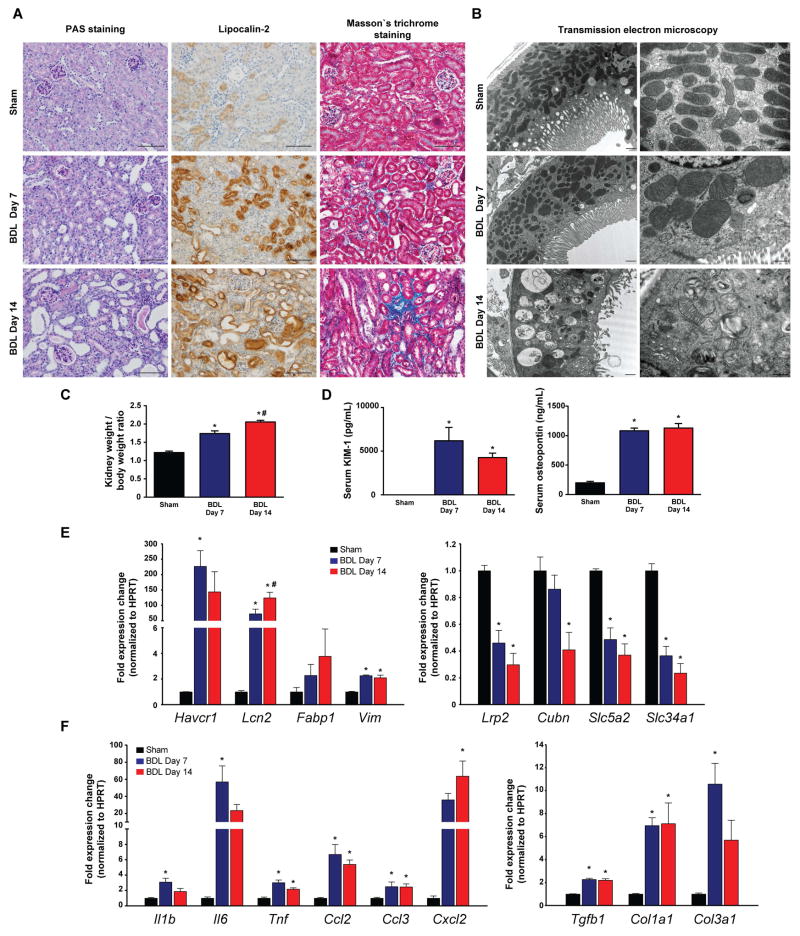
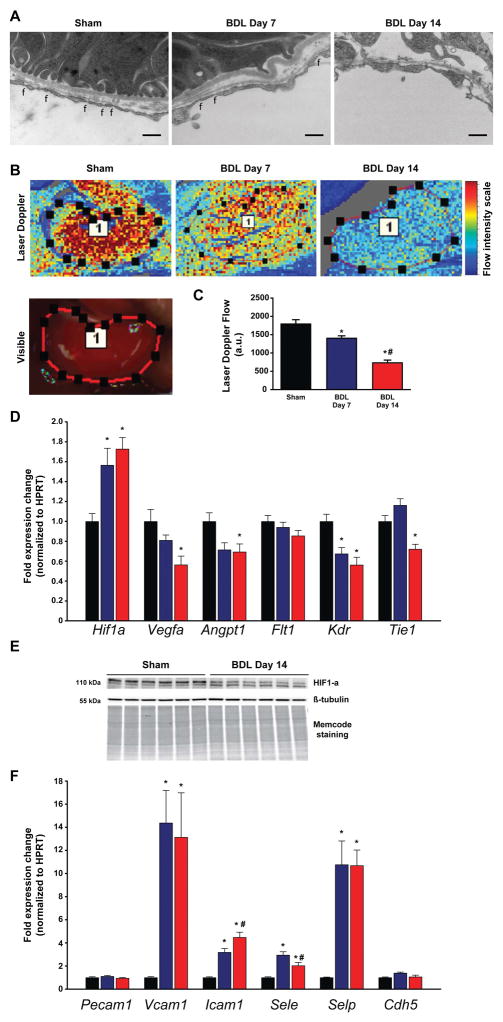
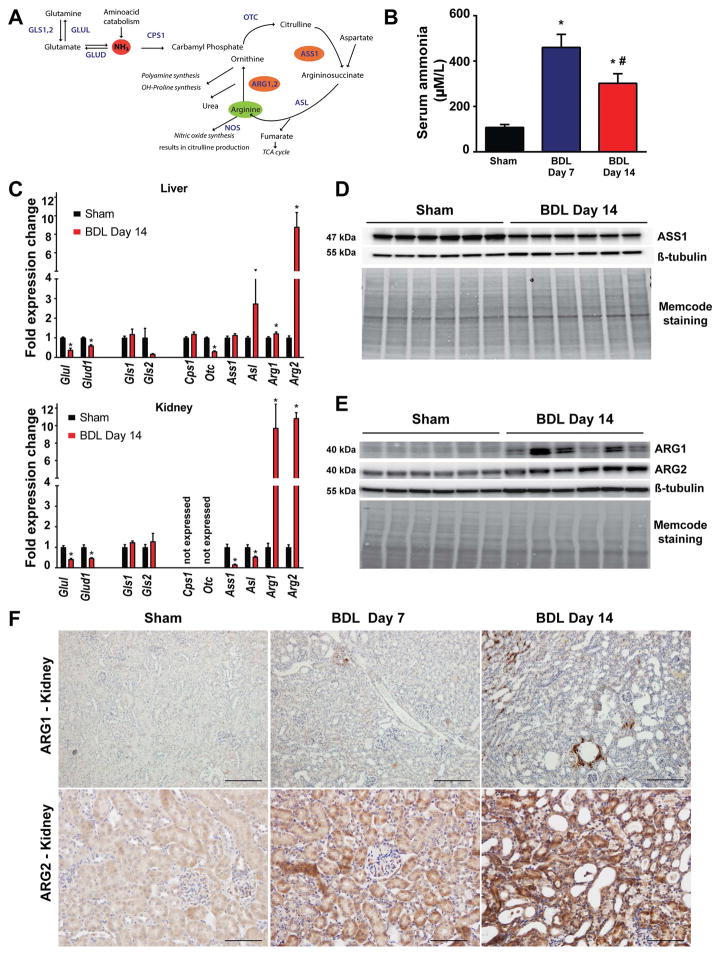
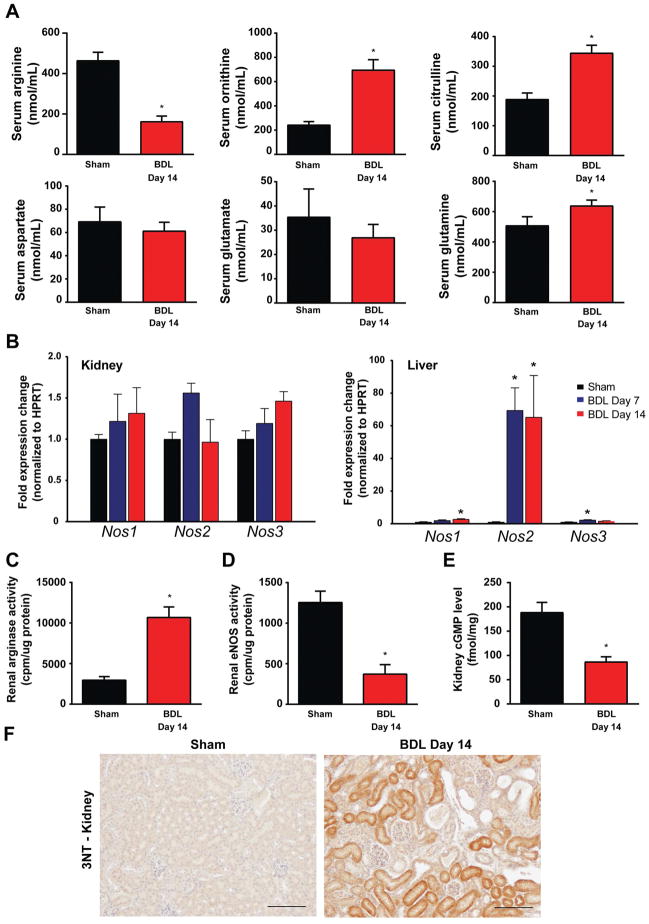
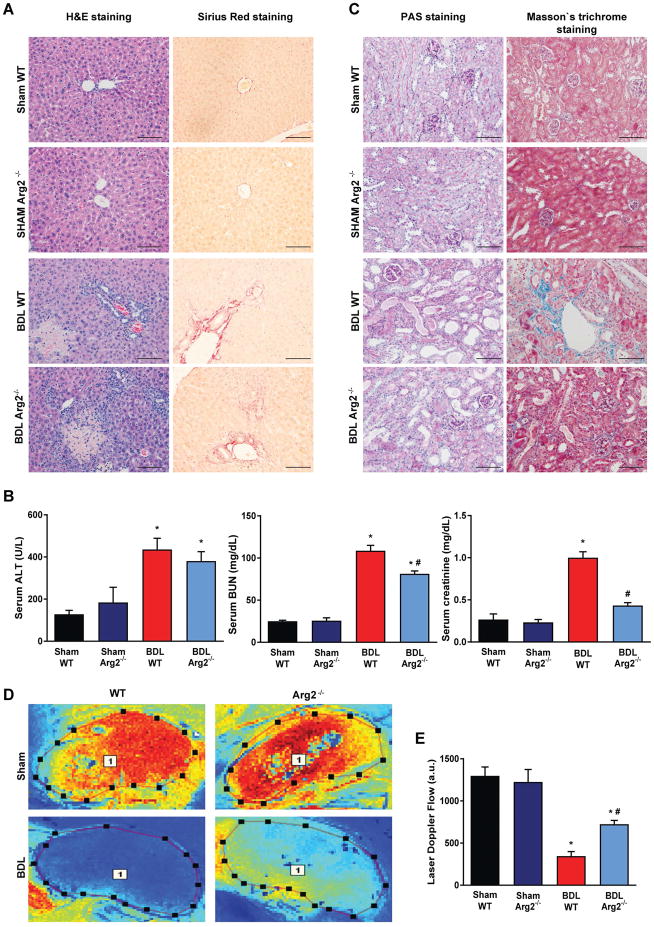
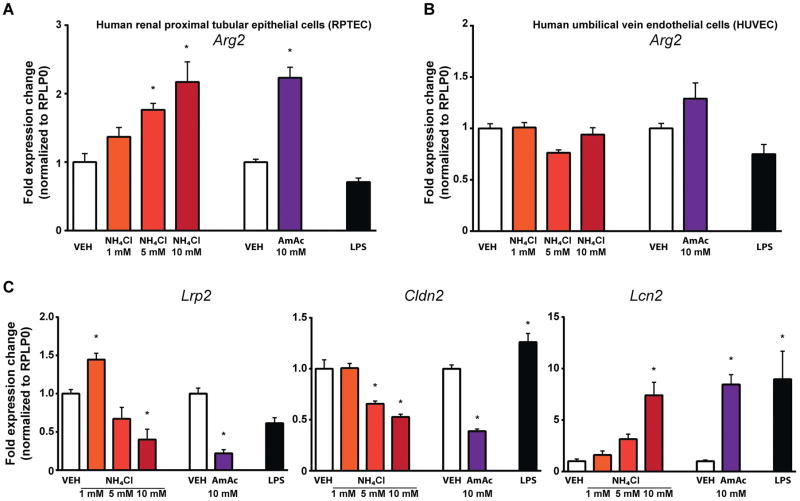
Tubular dysfunction is an important feature of renal injury in hepatorenal syndrome (HRS) in patients with end-stage liver disease. The pathogenesis of kidney injury in HRS is elusive, and there are no clinically relevant rodent models of HRS. We investigated the renal consequences of bile duct ligation (BDL)-induced hepatic and renal injury in mice in vivo by using biochemical assays, real-time polymerase chain reaction (PCR), Western blot, mass spectrometry, histology, and electron microscopy. BDL resulted in time-dependent hepatic injury and hyperammonemia which were paralleled by tubular dilation and tubulointerstitial nephritis with marked upregulation of lipocalin-2, kidney injury molecule 1 (KIM-1) and osteopontin. Renal injury was associated with dramatically impaired microvascular flow and decreased endothelial nitric oxide synthase (eNOS) activity. Gene expression analyses signified proximal tubular epithelial injury, tissue hypoxia, inflammation, and activation of the fibrotic gene program. Marked changes in renal arginine metabolism (upregulation of arginase-2 and downregulation of argininosuccinate synthase 1), resulted in decreased circulating arginine levels. Arginase-2 knockout mice were partially protected from BDL-induced renal injury and had less impairment in microvascular function. In human-cultured proximal tubular epithelial cells hyperammonemia per se induced upregulation of arginase-2 and markers of tubular cell injury.
Conclusion: We propose that hyperammonemia may contribute to impaired renal arginine metabolism, leading to decreased eNOS activity, impaired microcirculation, tubular cell death, tubulointerstitial nephritis and fibrosis. Genetic deletion of arginase-2 partially restores microcirculation and thereby alleviates tubular injury. We also demonstrate that BDL in mice is an excellent, clinically relevant model to study the renal consequences of HRS. (Hepatology 2018; 00:000-000).
© 2018 by the American Association for the Study of Liver Diseases.
Conflict of interest statement
Figures
References
-
- Blachier M, Leleu H, Peck-Radosavljevic M, Valla DC, Roudot-Thoraval F. The burden of liver disease in Europe: a review of available epidemiological data. J Hepatol. 2013;58:593–608. - PubMed
-
- Pericleous M, Sarnowski A, Moore A, Fijten R, Zaman M. The clinical management of abdominal ascites, spontaneous bacterial peritonitis and hepatorenal syndrome: a review of current guidelines and recommendations. Eur J Gastroenterol Hepatol. 2016;28:e10–18. - PubMed
-
- Davenport A, Sheikh MF, Lamb E, Agarwal B, Jalan R. Acute kidney injury in acute-on-chronic liver failure: where does hepatorenal syndrome fit? Kidney Int. 2017;92(5):1058–1070. - PubMed
-
- Garcia-Tsao G, Parikh CR, Viola A. Acute kidney injury in cirrhosis. Hepatology. 2008;48:2064–2077. - PubMed
-
- Cardenas A, Gines P, Uriz J, Bessa X, Salmeron JM, Mas A, Ortega R, et al. Renal failure after upper gastrointestinal bleeding in cirrhosis: incidence, clinical course, predictive factors, and short-term prognosis. Hepatology. 2001;34:671–676. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
