

Noninvasive diagnostic adjuncts for the evaluation of potentially premalignant oral epithelial lesions: current limitations and future directions
- PMID: 29631985
- PMCID: PMC6083875
- DOI: 10.1016/j.oooo.2018.02.020
Noninvasive diagnostic adjuncts for the evaluation of potentially premalignant oral epithelial lesions: current limitations and future directions
Abstract
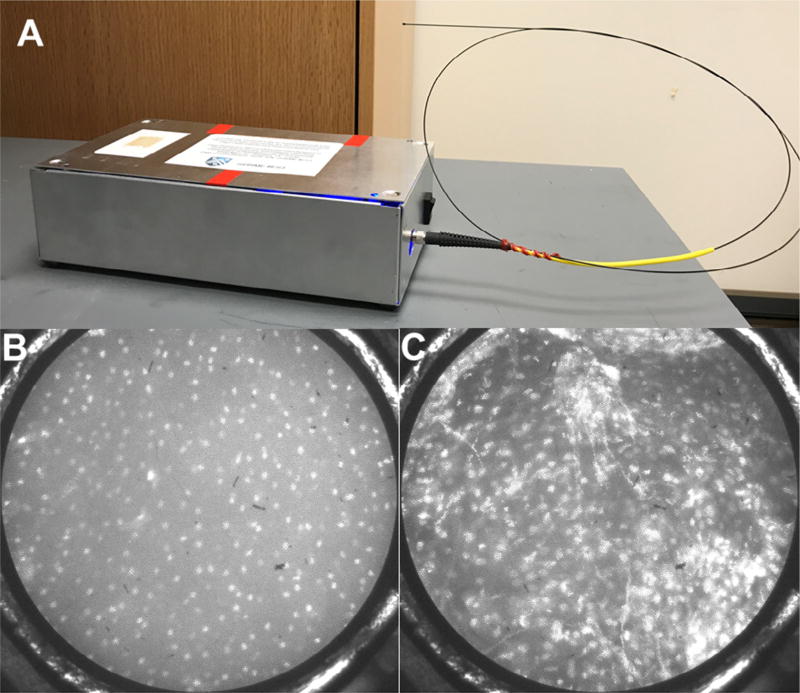
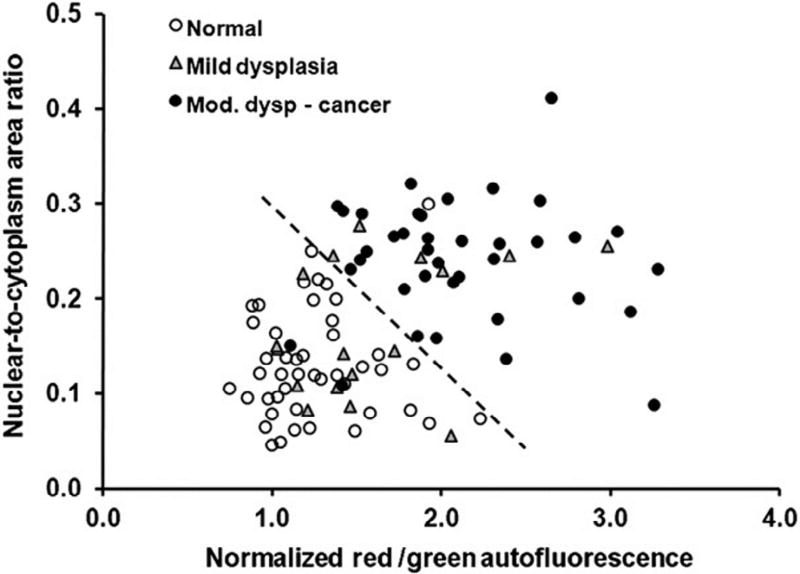
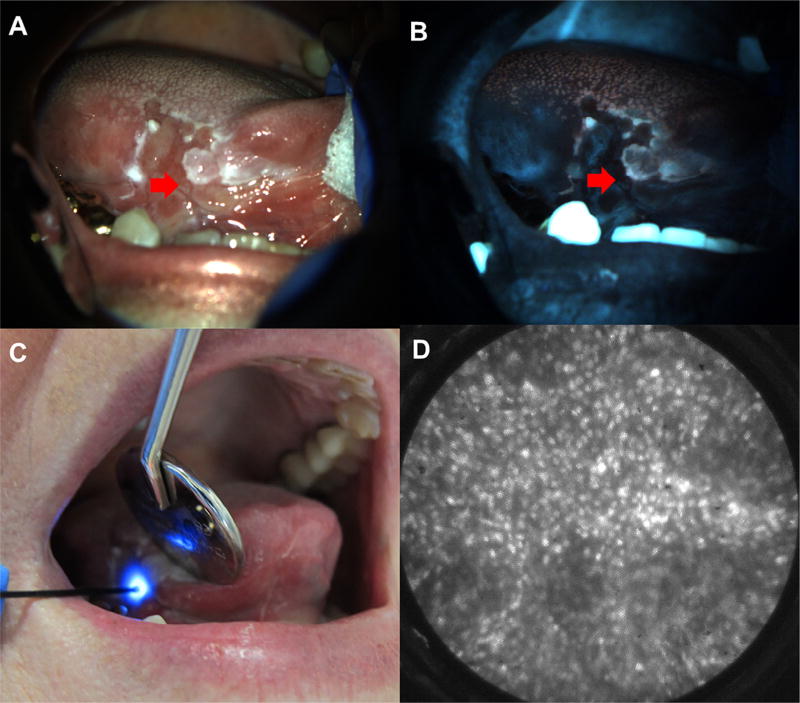
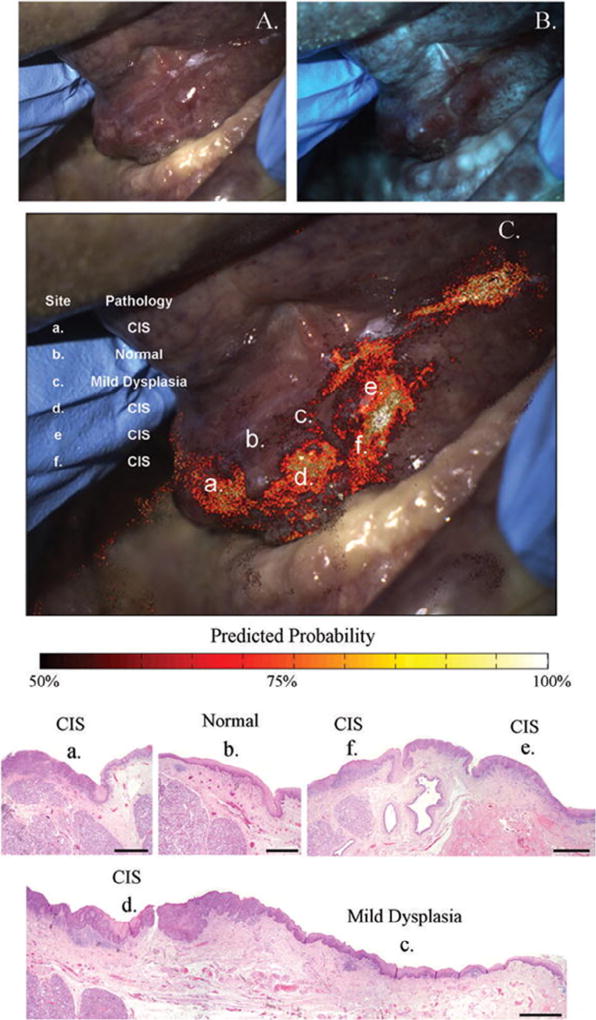
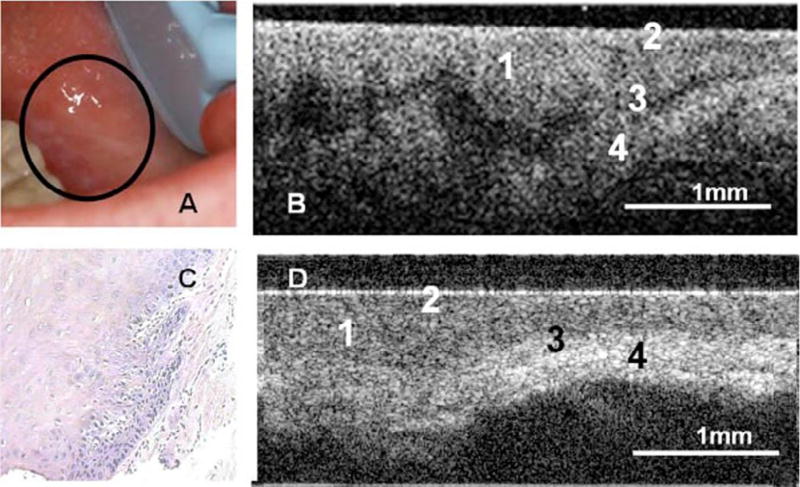
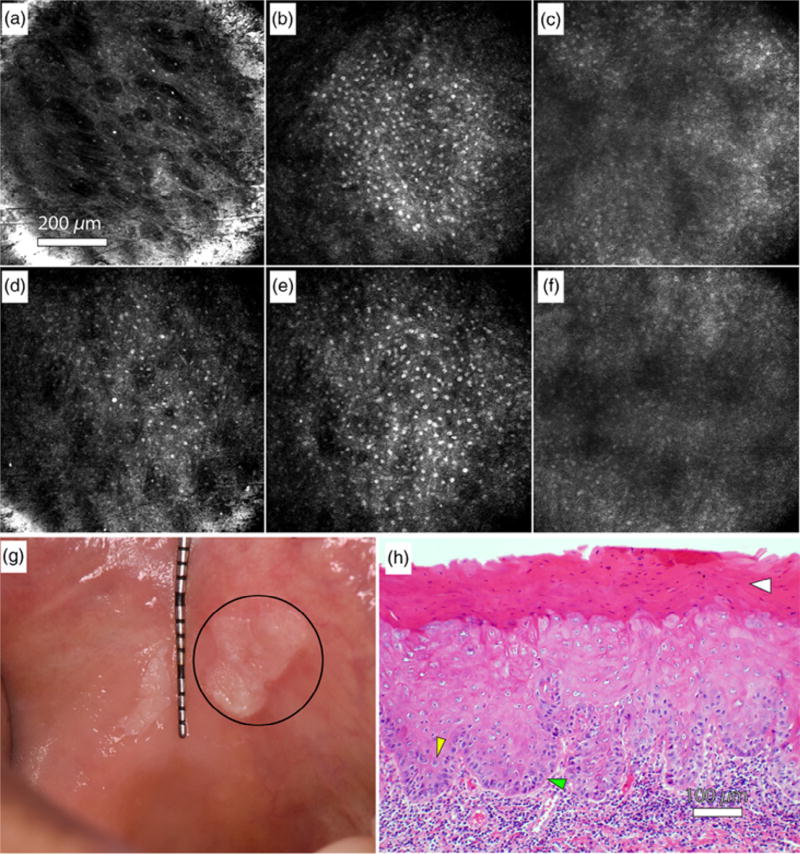
Potentially premalignant oral epithelial lesions (PPOELs) are a group of clinically suspicious conditions, of which a small percentage will undergo malignant transformation. PPOELs are suboptimally diagnosed and managed under the current standard of care. Dysplasia is the most well-established marker to distinguish high-risk PPOELs from low-risk PPOELs, and performing a biopsy to establish dysplasia is the diagnostic gold standard. However, a biopsy is limited by morbidity, resource requirements, and the potential for underdiagnosis. Diagnostic adjuncts may help clinicians better evaluate PPOELs before definitive biopsy, but existing adjuncts, such as toluidine blue, acetowhitening, and autofluorescence imaging, have poor accuracy and are not generally recommended. Recently, in vivo microscopy technologies, such as high-resolution microendoscopy, optical coherence tomography, reflectance confocal microscopy, and multiphoton imaging, have shown promise for improving PPOEL patient care. These technologies allow clinicians to visualize many of the same microscopic features used for histopathologic assessment at the point of care.
Copyright © 2018 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386. - PubMed
-
- Warnakulasuriya S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009;45:309–316. - PubMed
-
- Warnakulasuriya S, Johnson NW, Van Der Waal I. Nomenclature and classification of potentially malignant disorders of the oral mucosa. J Oral Pathol Med. 2007;36:575–580. - PubMed
-
- Warnakulasuriya S, Ariyawardana A. Malignant transformation of oral leukoplakia: a systematic review of observational studies. J Oral Pathol Med. 2016;45:155–166. - PubMed
-
- Bouquot JE, Speight PM, Farthing PM. Epithelial dysplasia of the oral mucosa—diagnostic problems and prognostic features. Curr Diagn Pathol. 2006;12:11–21.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
