

A randomised controlled trial of a facilitated home-based rehabilitation intervention in patients with heart failure with preserved ejection fraction and their caregivers: the REACH-HFpEF Pilot Study
- PMID: 29632081
- PMCID: PMC5893929
- DOI: 10.1136/bmjopen-2017-019649
A randomised controlled trial of a facilitated home-based rehabilitation intervention in patients with heart failure with preserved ejection fraction and their caregivers: the REACH-HFpEF Pilot Study
Erratum in
-
Correction: A randomised controlled trial of a facilitated home-based rehabilitation intervention in patients with heart failure with preserved ejection fraction and their caregivers: the REACH-HFpEF Pilot Study.BMJ Open. 2019 Mar 23;9(3):e019649corr1. doi: 10.1136/bmjopen-2017-019649corr1. BMJ Open. 2019. PMID: 30904881 Free PMC article. No abstract available.
Abstract
Introduction: Home-based cardiac rehabilitation may overcome suboptimal rates of participation. The overarching aim of this study was to assess the feasibility and acceptability of the novel Rehabilitation EnAblement in CHronic Hear Failure (REACH-HF) rehabilitation intervention for patients with heart failure with preserved ejection fraction (HFpEF) and their caregivers.
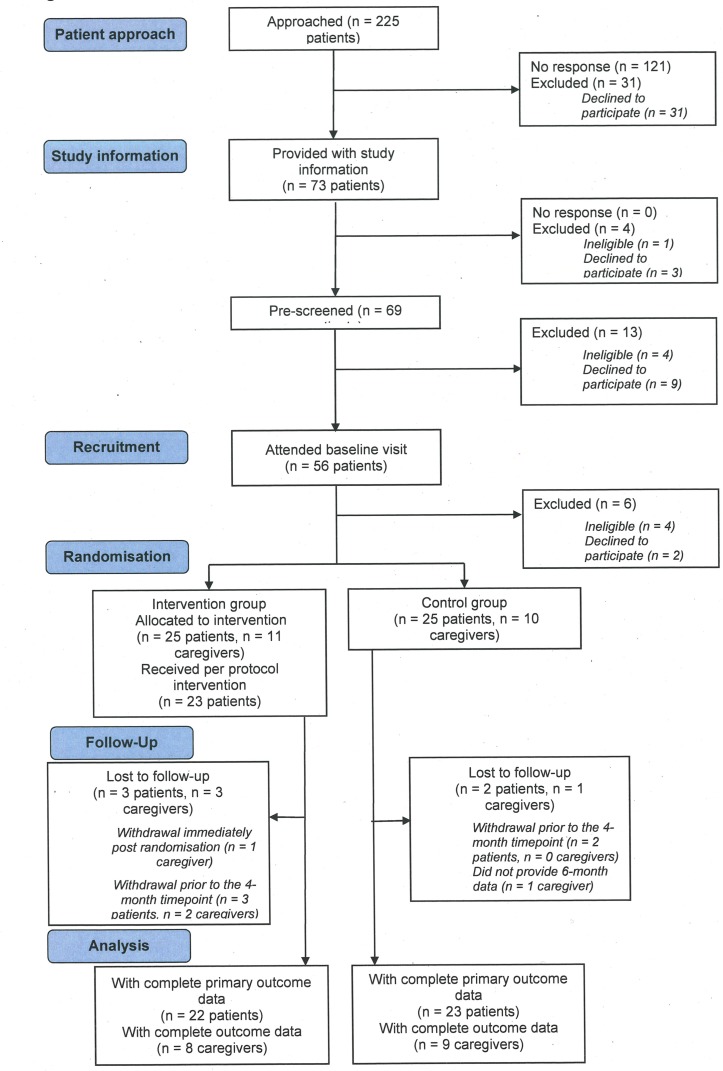
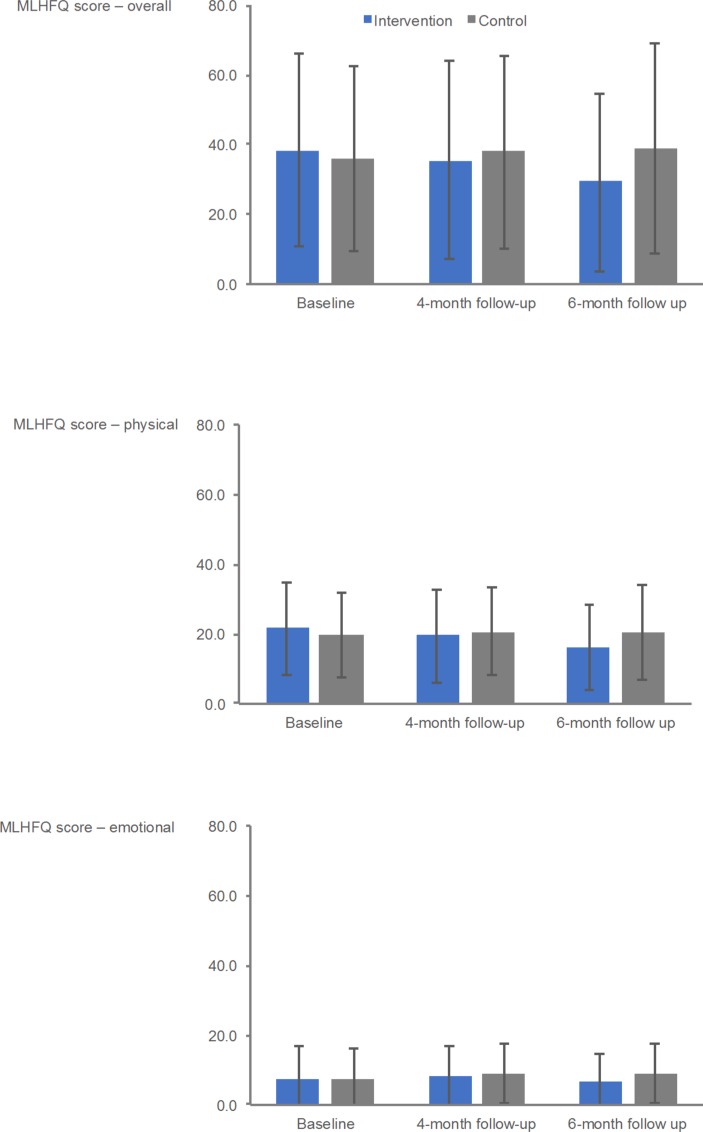
Methods and results: Patients were randomised 1:1 to REACH-HF intervention plus usual care (intervention group) or usual care alone (control group). REACH-HF is a home-based comprehensive self-management rehabilitation programme that comprises patient and carer manuals with supplementary tools, delivered by trained healthcare facilitators over a 12 week period. Patient outcomes were collected by blinded assessors at baseline, 3 months and 6 months postrandomisation and included health-related quality of life (primary) and psychological well-being, exercise capacity, physical activity and HF-related hospitalisation (secondary). Outcomes were also collected in caregivers.We enrolled 50 symptomatic patients with HF from Tayside, Scotland with a left ventricular ejection fraction ≥45% (mean age 73.9 years, 54% female, 100% white British) and 21 caregivers. Study retention (90%) and intervention uptake (92%) were excellent. At 6 months, data from 45 patients showed a potential direction of effect in favour of the intervention group, including the primary outcome of Minnesota Living with Heart Failure Questionnaire total score (between-group mean difference -11.5, 95% CI -22.8 to 0.3). A total of 11 (4 intervention, 7 control) patients experienced a hospital admission over the 6 months of follow-up with 4 (control patients) of these admissions being HF-related. Improvements were seen in a number intervention caregivers' mental health and burden compared with control.
Conclusions: Our findings support the feasibility and rationale for delivering the REACH-HF facilitated home-based rehabilitation intervention for patients with HFpEF and their caregivers and progression to a full multicentre randomised clinical trial to test its clinical effectiveness and cost-effectiveness.
Trial registration number: ISRCTN78539530.
Keywords: cardiac rehabilitation; caregivers; complex intervention; heart failure; heart failure with preserved ejection fraction; randomised controlled trial.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: RST is the lead for the ongoing portfolio of Cochrane reviews of cardiac rehabilitation. RST and HMD are named Scientific Advisors for the ongoing National Institute of Health and Care Excellence (NICE) updated clinical guidelines for the management heart failure (CG108). HMD is an ordinary member of the British Association for Cardiovascular Prevention and Rehabilitation (BACPR) council. All other coauthors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous