

Estimating the health and economic effects of the proposed US Food and Drug Administration voluntary sodium reformulation: Microsimulation cost-effectiveness analysis
- PMID: 29634725
- PMCID: PMC5892867
- DOI: 10.1371/journal.pmed.1002551
Estimating the health and economic effects of the proposed US Food and Drug Administration voluntary sodium reformulation: Microsimulation cost-effectiveness analysis
Abstract
Background: Sodium consumption is a modifiable risk factor for higher blood pressure (BP) and cardiovascular disease (CVD). The US Food and Drug Administration (FDA) has proposed voluntary sodium reduction goals targeting processed and commercially prepared foods. We aimed to quantify the potential health and economic impact of this policy.
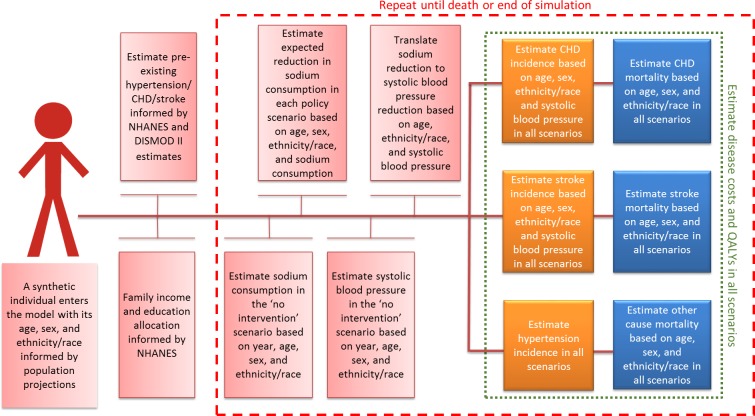
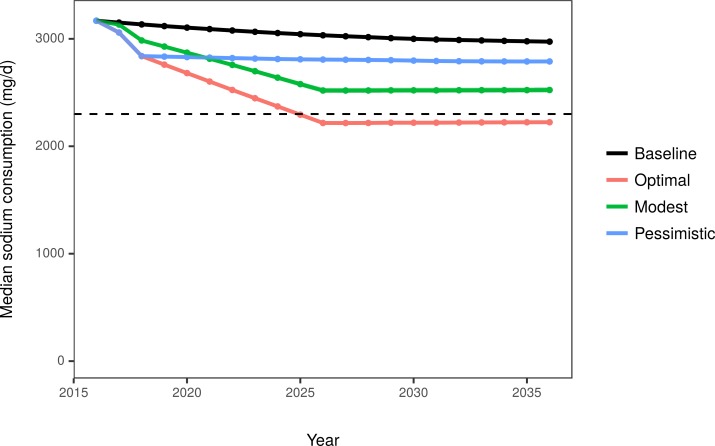
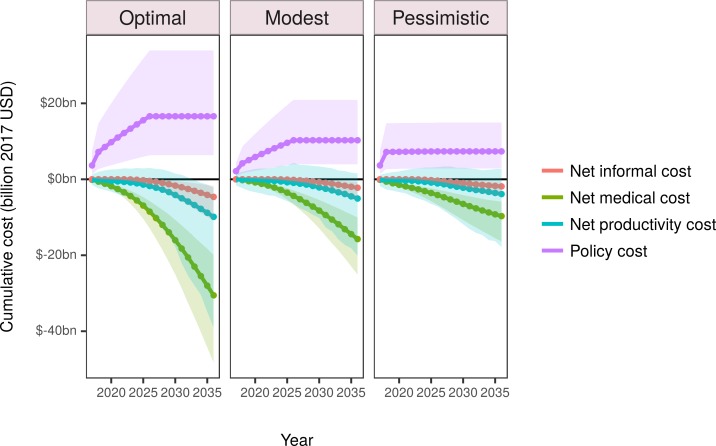
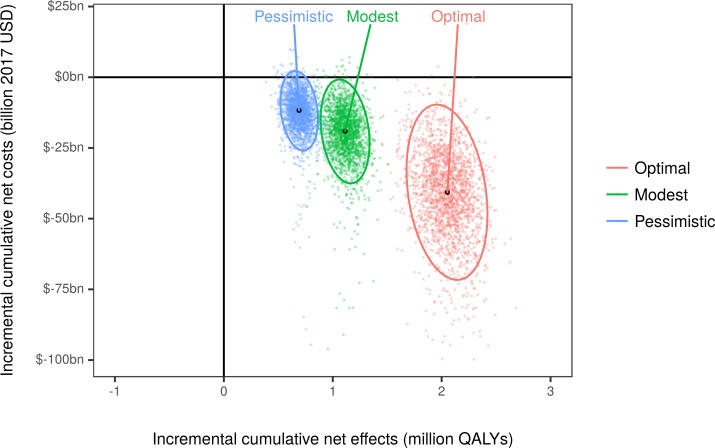
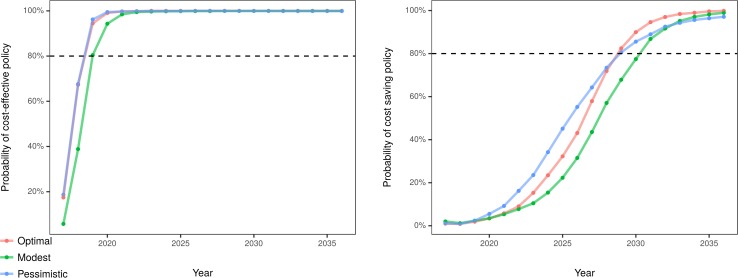
Methods and findings: We used a microsimulation approach of a close-to-reality synthetic population (US IMPACT Food Policy Model) to estimate CVD deaths and cases prevented or postponed, quality-adjusted life years (QALYs), and cost-effectiveness from 2017 to 2036 of 3 scenarios: (1) optimal, 100% compliance with 10-year reformulation targets; (2) modest, 50% compliance with 10-year reformulation targets; and (3) pessimistic, 100% compliance with 2-year reformulation targets, but with no further progress. We used the National Health and Nutrition Examination Survey and high-quality meta-analyses to inform model inputs. Costs included government costs to administer and monitor the policy, industry reformulation costs, and CVD-related healthcare, productivity, and informal care costs. Between 2017 and 2036, the optimal reformulation scenario achieving the FDA sodium reduction targets could prevent approximately 450,000 CVD cases (95% uncertainty interval: 240,000 to 740,000), gain approximately 2.1 million discounted QALYs (1.7 million to 2.4 million), and produce discounted cost savings (health savings minus policy costs) of approximately $41 billion ($14 billion to $81 billion). In the modest and pessimistic scenarios, health gains would be 1.1 million and 0.7 million QALYS, with savings of $19 billion and $12 billion, respectively. All the scenarios were estimated with more than 80% probability to be cost-effective (incremental cost/QALY < $100,000) by 2021 and to become cost-saving by 2031. Limitations include evaluating only diseases mediated through BP, while decreasing sodium consumption could have beneficial effects upon other health burdens such as gastric cancer. Further, the effect estimates in the model are based on interventional and prospective observational studies. They are therefore subject to biases and confounding that may have influenced also our model estimates.
Conclusions: Implementing and achieving the FDA sodium reformulation targets could generate substantial health gains and net cost savings.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: LW is employed by the American Heart Association as Director of Policy Research. RM reports grants from NIH during the conduct of the study. In addition, RM is a PI of a research grant from Unilever on an investigator-initiated project to assess the effects of omega-6 fatty acid biomarkers on diabetes and heart disease, and reports personal fees from the World Bank and Bunge; all outside the submitted work. DM reports honoraria or consulting from Astra Zeneca, Acasti Pharma, GOED, DSM, Haas Avocado Board, Nutrition Impact, Pollock Communications, Boston Heart Diagnostics, and Bunge. DM also is on the scientific advisory board for Omada Health and Elysium Health, receives chapter royalties from UpToDate, and also receives research funding from NIH and the Gates Foundation. JPS reports personal fees from ICF strategic consulting outside of the submitted work.
Figures
References
-
- Micha R, Penalvo JL, Cudhea F, Imamura F, Rehm CD, Mozaffarian D. association between dietary factors and mortality from heart disease, stroke, and type 2 diabetes in the United States. JAMA. 2017;317(9):912–24. doi: 10.1001/jama.2017.0947 - DOI - PMC - PubMed
-
- Mozaffarian D, Fahimi S, Singh GM, Micha R, Khatibzadeh S, Engell RE, et al. Global sodium consumption and death from cardiovascular causes. N Engl J Med. 2014;371(7):624–34. doi: 10.1056/NEJMoa1304127 - DOI - PubMed
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke statistics—2016 update: a report from the American Heart Association. Circulation. 2016;133(4):e38–360. doi: 10.1161/CIR.0000000000000350 - DOI - PubMed
-
- Khavjou O, Phelps D, Leib A. Projections of cardiovascular disease prevalence and costs: 2015–2035. Dallas: American Heart Association; 2016. [cited 2018 Mar 12]. Available from: http://www.heart.org/idc/groups/ahaecc-public/@wcm/@global/documents/dow....
-
- Dietary Guidelines Advisory Committee. Scientific report of the 2015 Dietary Guidelines Advisory Committee Washington (DC): US Department of Health and Human Services; 2015. [cited 2018 Mar 12]. Available from: http://health.gov/dietaryguidelines/2015-scientific-report/pdfs/scientif....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
