

Folate Receptor Near-Infrared Optical Imaging Provides Sensitive and Specific Intraoperative Visualization of Nonfunctional Pituitary Adenomas
- PMID: 29635300
- PMCID: PMC7189272
- DOI: 10.1093/ons/opy034
Folate Receptor Near-Infrared Optical Imaging Provides Sensitive and Specific Intraoperative Visualization of Nonfunctional Pituitary Adenomas
Abstract
Background: Surgical resection is the primary treatment for nonfunctional (NF) pituitary adenomas, but gross-total resection is difficult to achieve in all cases. NF adenomas overexpress folate receptor alpha (FRα).
Objective: To test the hypothesis that we could target FRα for highly sensitive and specific intraoperative detection of NF adenomas using near-infrared (NIR) imaging.
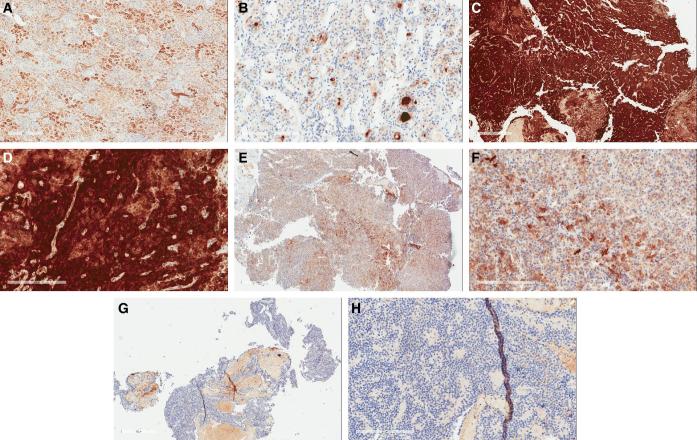
Methods: Fourteen patients with NF pituitary adenoma were infused with the folate analog NIR dye OTL38 preoperatively. NIR fluorescence signal-to-background ratio (SBR) was recorded for each tumor during resection of the adenomas. Extent of surgery was not modified based on the presence or absence of fluorescence. Immunohistochemistry was performed to assess FRα expression in all specimens. Magnetic resonance imaging (MRI) was performed postoperatively to assess residual neoplasm.
Results: Nine adenomas overexpressed FRα and fluoresced with a NIR SBR of 3.2 ± 0.52, whereas the 5 non-FRα-overexpressing adenomas fluoresced with an SBR of 1.5 ± 0.21. Linear regression demonstrated a significant correlation between intraoperative SBR and the FRα expression (P-value < .001). Analysis of 14 margin samples revealed that the surgeon's impression of the tissue had 83% sensitivity, 100% specificity, 100% positive predictive value, and 89% negative predictive value, while NIR fluorescence had 100% for all values. NIR fluorescence accurately predicted postoperative MRI results in 78% of FRα-overexpressing patients.
Conclusion: Preoperative injection of folate-tagged NIR dye provides strong signal and visualization of NF pituitary adenomas. It is 100% sensitive and specific for detecting margin neoplasm and can predict postoperative MRI findings. Our results suggest that NIR fluorescence may be superior to white-light visualization alone and may improve resection rates in NF pituitary adenomas.
Figures




References
-
- Ezzat S, Asa SL, Couldwell WTet al.. The prevalence of pituitary adenomas. Cancer. 2004;101(3):613-619. - PubMed
-
- Greenman Y, Cooper O, Yaish Iet al.. Treatment of clinically nonfunctioning pituitary adenomas with dopamine agonists. Eur J Endocrinol. 2016;175(1):63-72. - PubMed
-
- Lee JYK, Bohman L-E, Bergsneider M. Contemporary neurosurgical techniques for pituitary tumor resection. J Neurooncol. 2014;117(3):437-444. - PubMed
-
- Losa M, Mortini P, Barzaghi Ret al.. Early results of surgery in patients with nonfunctioning pituitary adenoma and analysis of the risk of tumor recurrence. J Neurosurg. 2008;108(3):525-532. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
