

Perspective: Protein Requirements and Optimal Intakes in Aging: Are We Ready to Recommend More Than the Recommended Daily Allowance?
- PMID: 29635313
- PMCID: PMC5952928
- DOI: 10.1093/advances/nmy003
Perspective: Protein Requirements and Optimal Intakes in Aging: Are We Ready to Recommend More Than the Recommended Daily Allowance?
Abstract
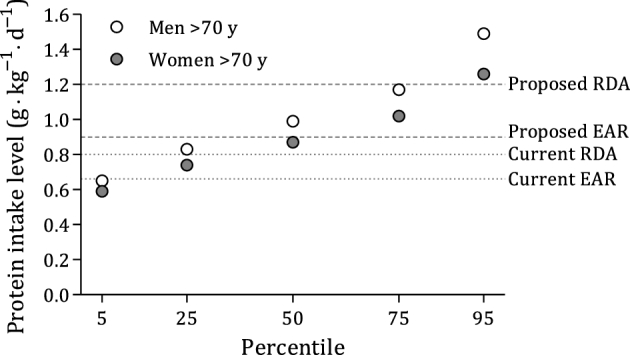
The Dietary Reference Intakes set the protein RDA for persons >19 y of age at 0.8 g protein ⋅ kg body weight-1 ⋅ d-1. A growing body of evidence suggests, however, that the protein RDA may be inadequate for older individuals. The evidence for recommending a protein intake greater than the RDA comes from a variety of metabolic approaches. Methodologies centered on skeletal muscle are of paramount importance given the age-related decline in skeletal muscle mass and function (sarcopenia) and the degree to which dietary protein could mitigate these declines. In addition to evidence from short-term experimental trials, observational data show that higher protein intakes are associated with greater muscle mass and, more importantly, better muscle function with aging. We are in dire need of more evidence from longer-term intervention trials showing the efficacy of protein intakes that are higher than the RDA in older persons to support skeletal muscle health. We propose that it should be recommended that older individuals consume ≥1.2 g protein · kg-1 · d-1 and that there should be an emphasis on the intake of the amino acid leucine, which plays a central role in stimulating skeletal muscle anabolism. Critically, the often-cited potential negative effects of consuming higher protein intakes on renal and bone health are without a scientific foundation in humans.
Figures
References
-
- Janssen I. Evolution of sarcopenia research. Appl Physiol Nutr Metab 2010;35(5):707–12. - PubMed
-
- Rosenthal MD, Glew RH. Medical biochemistry. Hoboken (NJ): John Wiley & Sons, Inc.; 2009.
-
- Janssen I, Shepard DS, Katzmarzyk PT, Roubenoff R. The healthcare costs of sarcopenia in the United States. J Am Geriatr Soc 2004;52(1):80–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
