

Sarcopenic obesity assessed using dual energy X-ray absorptiometry (DXA) can predict cardiovascular disease in patients with type 2 diabetes: a retrospective observational study
- PMID: 29636045
- PMCID: PMC5891961
- DOI: 10.1186/s12933-018-0700-5
Sarcopenic obesity assessed using dual energy X-ray absorptiometry (DXA) can predict cardiovascular disease in patients with type 2 diabetes: a retrospective observational study
Abstract
Background: Sarcopenic obesity, defined as reduced skeletal muscle mass and power with increased adiposity, was reported to be associated with cardiovascular disease risks in previous cross-sectional studies. Whole body dual-energy X-ray absorptiometry (DXA) can simultaneously evaluate both fat and muscle mass, therefore, whole body DXA may be suitable for the diagnosis of sarcopenic obesity. However, little is known regarding whether sarcopenic obesity determined using whole body DXA could predict incident cardiovascular disease (CVD). The aim of this study was to investigate the impact of sarcopenic obesity on incident CVD in patients with type 2 diabetes.
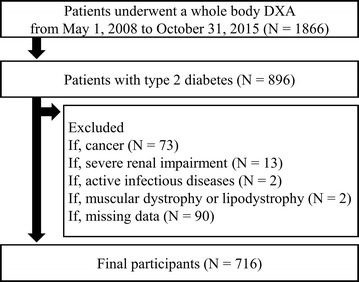
Methods: A total of 716 Japanese patients (mean age 65 ± 13 years; 47.0% female) were enrolled. Android fat mass (kg), gynoid fat mass (kg), and skeletal muscle index (SMI) calculated as appendicular non-fat mass (kg) divided by height squared (m2), were measured using whole body DXA. Sarcopenic obesity was defined as the coexistence of low SMI and obesity determined by four patterns of obesity as follows: android to gynoid ratio (A/G ratio), android fat mass or percentage of body fat (%BF) was higher than the sex-specific median, or body mass index (BMI) was equal to or greater than 25 kg/m2. The study endpoint was the first occurrence or recurrence of CVD.
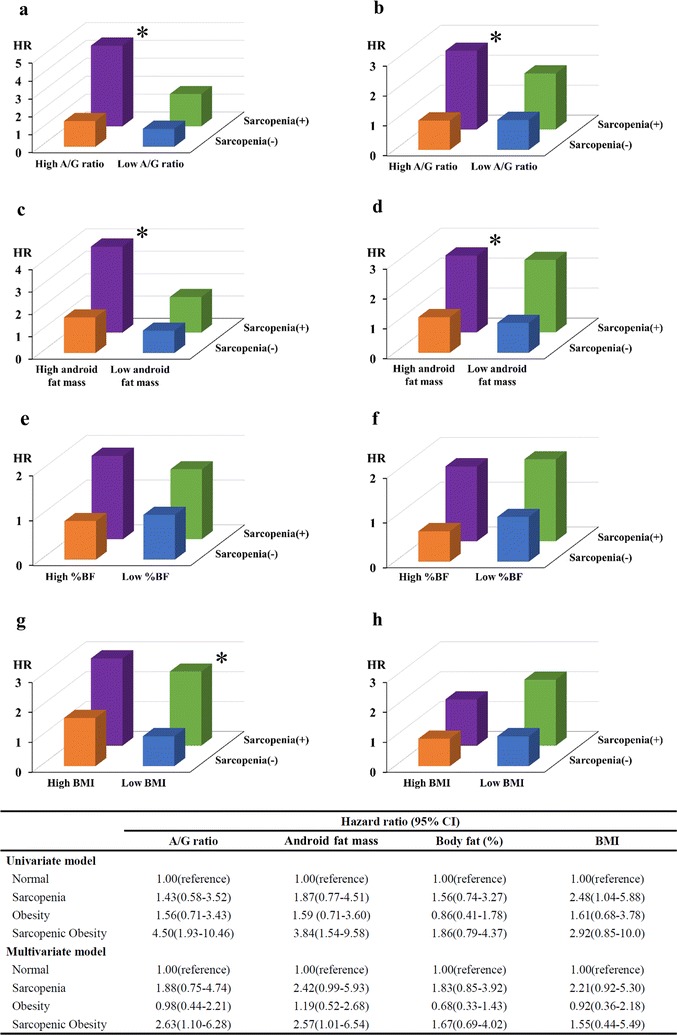
Results: Over a median follow up of 2.6 years (IQR 2.1-3.2 years), 53 patients reached the endpoint. Sarcopenic obesity was significantly associated with incident CVD even after adjustment for the confounding variables, when using A/G ratio [hazard ratio (HR) 2.63, 95% CI 1.10-6.28, p = 0.030] and android fat mass (HR 2.57, 95% CI 1.01-6.54, p = 0.048) to define obesity, but not %BF (HR 1.67, 95% CI 0.69-4.02, p = 0.252), and BMI (HR 1.55, 95% CI 0.44-5.49, p = 0.496).
Conclusions: The present data suggest that the whole body DXA is valuable in the diagnosis of sarcopenic obesity (high A/G ratio or android fat mass with low SMI) to determine the risk of CVD events in patients with type 2 diabetes. Meanwhile, sarcopenic obesity classified with low SMI, and high %BF or BMI was not associated with incident CVD.
Keywords: Cardiovascular disease; Dual-energy X-ray absorptiometry; Sarcopenic obesity; Type 2 diabetes; Visceral adiposity.
Figures
References
-
- Canoy D, Boekholdt SM, Wareham N, Luben R, Welch A, Bingham S, Buchan I, Day N, Khaw KT. Body fat distribution and risk of coronary heart disease in men and women in the European Prospective Investigation Into Cancer and Nutrition in Norfolk cohort: a population-based prospective study. Circulation. 2007;116:2933–2943. doi: 10.1161/CIRCULATIONAHA.106.673756. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
