

Role of lymph node dissection in the management of upper tract urothelial carcinomas: a meta-analysis
- PMID: 29636103
- PMCID: PMC5894184
- DOI: 10.1186/s12894-018-0336-5
Role of lymph node dissection in the management of upper tract urothelial carcinomas: a meta-analysis
Abstract
Background: Lymph node dissection (LND) is not routinely performed during radical nephroureterectomy (RNU) in upper tract urothelial carcinomas (UTUC) and the role of LND has been controversial. We aim to investigate whether patients with LND had improved survival in UTUC patients.
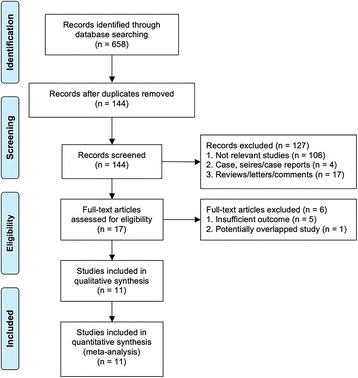
Methods: We performed a systematic literature search of PubMed, Embase, and Cochrane library for citations published prior to January 2016, describing LND performed among UTUC patients and conducted a standard meta-analysis of survival outcomes.
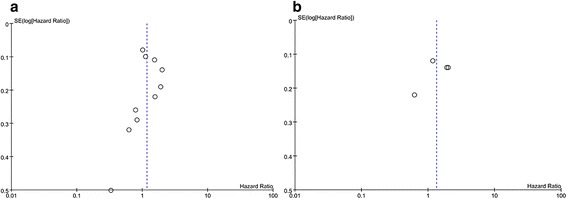
Results: Eleven eligible studies containing 7516 patients satisfied the inclusion criteria. Pooled HRs for cancer-specific survival (CSS) and recurrence-free survival (RFS) were 1.17 (P = 0.18) and 1.33 (P = 0.19) respectively. However, the patients in the LND group had more advanced tumour stages and grades (P < 0.001). Further subgroup analysis showed that among muscle-invasive UTUC patients, the pooled HR for CSS and RFS were 1.10 (P = 0.42) and 0.92 (P = 0.72) respectively. Besides, no difference was found in CSS and RFS between pN0 and pNx individuals in overall populations and in patients with muscle-invasive UTUC, while pN+ patients had significantly worse prognosis when compared to pN0 patients.
Conclusions: LND during RNU allows more accurate staging and prediction of survival, but it remains uncertain whether LND independently improves survival in patients with UTUC. However, standard use of LND should be further investigated in a multi-center, prospective evaluation to obtain a definitive statement regarding this matter.
Keywords: Lymph node dissection; Recurrence; Survival; Upper urinary tract; Urothelial carcinoma.
Conflict of interest statement
Competing interest
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2009). Produced by bob Phillips, Chris ball, Dave Sackett, Doug Badenoch, Sharon Straus, Brian Haynes, Martin Dawes since November 1998. Updated by Jeremy Howick March 2009.
-
- Schatteman P, Chatzopoulos C, Assenmacher C, De Visscher L, Jorion JL, Blaze V, et al. Laparoscopic nephroureterectomy for upper urinary tract transitional cell carcinoma: results of a Belgian retrospective multicentre survey. Eur Urol. 2007;51:1633–1638. doi: 10.1016/j.eururo.2006.09.016. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
