

Environmental Subconcussive Injury, Axonal Injury, and Chronic Traumatic Encephalopathy
- PMID: 29636723
- PMCID: PMC5880887
- DOI: 10.3389/fneur.2018.00166
Environmental Subconcussive Injury, Axonal Injury, and Chronic Traumatic Encephalopathy
Abstract
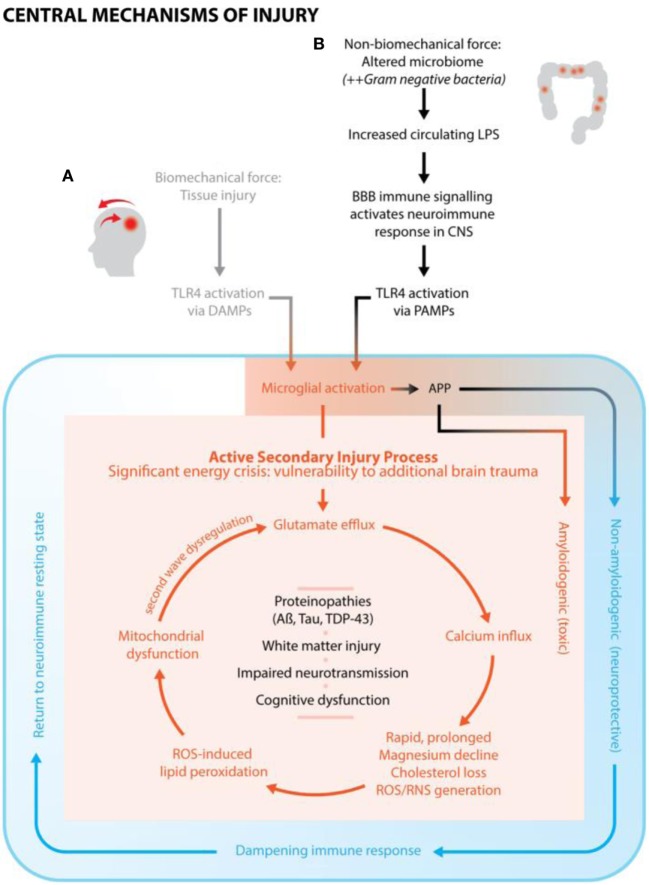
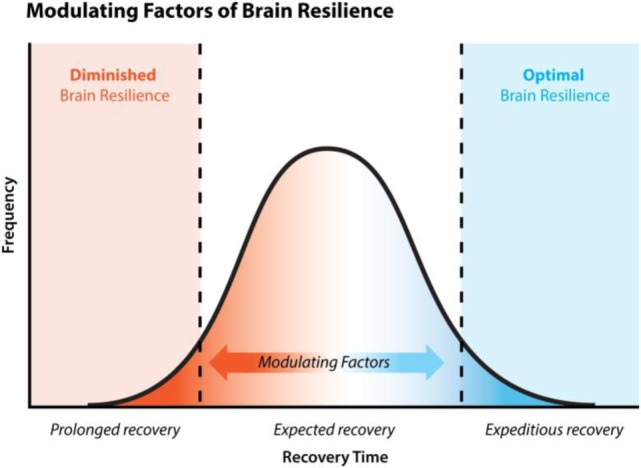
Brain injury occurs in two phases: the initial injury itself and a secondary cascade of precise immune-based neurochemical events. The secondary phase is typically functional in nature and characterized by delayed axonal injury with more axonal disconnections occurring than in the initial phase. Axonal injury occurs across the spectrum of disease severity, with subconcussive injury, especially when repetitive, now considered capable of producing significant neurological damage consistent with axonal injury seen in clinically evident concussion, despite no observable symptoms. This review is the first to introduce the concept of environmental subconcussive injury (ESCI) and sets out how secondary brain damage from ESCI once past the juncture of microglial activation appears to follow the same neuron-damaging pathway as secondary brain damage from conventional brain injury. The immune response associated with ESCI is strikingly similar to that mounted after conventional concussion. Specifically, microglial activation is followed closely by glutamate and calcium flux, excitotoxicity, reactive oxygen species and reactive nitrogen species (RNS) generation, lipid peroxidation, and mitochondrial dysfunction and energy crisis. ESCI damage also occurs in two phases, with the primary damage coming from microbiome injury (due to microbiome-altering events) and secondary damage (axonal injury) from progressive secondary neurochemical events. The concept of ESCI and the underlying mechanisms have profound implications for the understanding of chronic traumatic encephalopathy (CTE) etiology because it has previously been suggested that repetitive axonal injury may be the primary CTE pathogenesis in susceptible individuals and it is best correlated with lifetime brain trauma load. Taken together, it appears that susceptibility to brain injury and downstream neurodegenerative diseases, such as CTE, can be conceptualized as a continuum of brain resilience. At one end is optimal resilience, capable of launching effective responses to injury with spontaneous recovery, and at the other end is diminished resilience with a compromised ability to respond and/or heal appropriately. Modulating factors such as one's total cumulative and synergistic brain trauma load, bioavailability of key nutrients needed for proper functioning of restorative metabolic pathways (specifically those involved in the deactivation and clearance of metabolic by-products of brain injury) are key to ultimately determining one's brain resilience.
Keywords: axonal injury; chronic traumatic encephalopathy; environmental neurotoxins; lipopolysaccharide; subconcussion.
Figures
Similar articles
-
Chronic Traumatic Encephalopathy: The cellular sequela to repetitive brain injury.J Clin Neurosci. 2017 Jul;41:24-29. doi: 10.1016/j.jocn.2017.03.035. Epub 2017 Mar 27. J Clin Neurosci. 2017. PMID: 28347679 Review.
-
Chronic Traumatic Encephalopathy in Athletes Involved with High-impact Sports.J Vasc Interv Neurol. 2016 Oct;9(2):34-48. J Vasc Interv Neurol. 2016. PMID: 27829969 Free PMC article.
-
Neurological consequences of traumatic brain injuries in sports.Mol Cell Neurosci. 2015 May;66(Pt B):114-22. doi: 10.1016/j.mcn.2015.03.012. Epub 2015 Mar 12. Mol Cell Neurosci. 2015. PMID: 25770439 Review.
-
Traumatic brain injury (TBI) in collision sports: Possible mechanisms of transformation into chronic traumatic encephalopathy (CTE).Metabolism. 2019 Nov;100S:153943. doi: 10.1016/j.metabol.2019.07.007. Metabolism. 2019. PMID: 31610856 Review.
-
Post-traumatic neurodegeneration and chronic traumatic encephalopathy.Mol Cell Neurosci. 2015 May;66(Pt B):81-90. doi: 10.1016/j.mcn.2015.03.007. Epub 2015 Mar 7. Mol Cell Neurosci. 2015. PMID: 25758552 Review.
Cited by
-
Tau pathology in the medial temporal lobe of athletes with chronic traumatic encephalopathy: a chronic effects of neurotrauma consortium study.Acta Neuropathol Commun. 2019 Dec 12;7(1):207. doi: 10.1186/s40478-019-0861-9. Acta Neuropathol Commun. 2019. PMID: 31831066 Free PMC article.
-
Evaluation of the specificity of the central diagnostic criterion for chronic traumatic encephalopathy.Ir J Med Sci. 2019 Aug;188(3):993-998. doi: 10.1007/s11845-018-1943-6. Epub 2018 Nov 30. Ir J Med Sci. 2019. PMID: 30506345
-
Late contributions of repetitive head impacts and TBI to depression symptoms and cognition.Neurology. 2020 Aug 18;95(7):e793-e804. doi: 10.1212/WNL.0000000000010040. Epub 2020 Jun 26. Neurology. 2020. PMID: 32591472 Free PMC article.
-
Developing methods to detect and diagnose chronic traumatic encephalopathy during life: rationale, design, and methodology for the DIAGNOSE CTE Research Project.Alzheimers Res Ther. 2021 Aug 12;13(1):136. doi: 10.1186/s13195-021-00872-x. Alzheimers Res Ther. 2021. PMID: 34384490 Free PMC article.
-
Changes in volumetric and metabolic parameters relate to differences in exposure to sub-concussive head impacts.J Cereb Blood Flow Metab. 2020 Jul;40(7):1453-1467. doi: 10.1177/0271678X19862861. Epub 2019 Jul 15. J Cereb Blood Flow Metab. 2020. PMID: 31307284 Free PMC article.
References
-
- BU Research CTE Center. VA-BU-CLF Brain Bank. (2017). Available from: https://www.bu.edu/cte/our-research/brain-bank/ (Accessed: March 12, 2018).
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous