

Case Reports
doi: 10.1002/ccr3.1392.
eCollection 2018 Apr.
Epiconus syndrome induced only in the erect standing position in a patient with L1 compression fracture: a representative case report
Affiliations
- PMID: 29636937
- PMCID: PMC5889228
- DOI: 10.1002/ccr3.1392
Item in Clipboard
Case Reports
Epiconus syndrome induced only in the erect standing position in a patient with L1 compression fracture: a representative case report
Clin Case Rep.
.
Abstract
In daily practice, when CT or MRI does not show a pathological lesion in a patient with persistent abnormal neurological signs, it is important to obtain imaging studies of the spine in dynamic position.
Keywords: Epiconus syndrome; expandable cage; myelography; neurological pathology; thoracolumbar spine; vertebral body fracture.
Figures
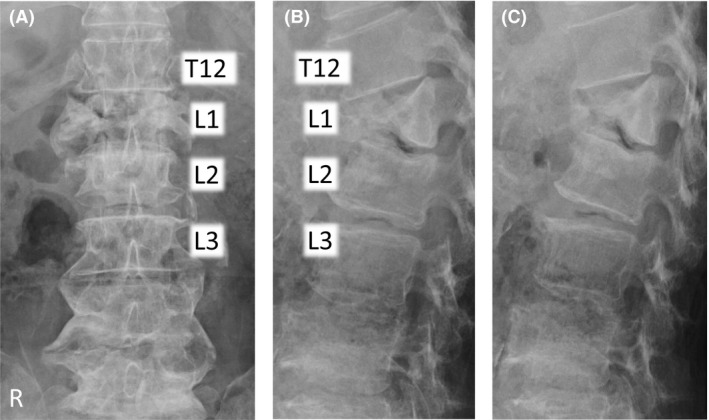
Plain radiographs in decubitus position. (A) Anteroposterior view, (B) lateral view in the flexion position, and (C) lateral view in the extension position on plain radiography performed on the examination table. These showed an L1 vertebral body fracture with an intact posterior wall. Flexion and extension views in the decubitus position showed no obvious malalignment of the vertebrae. Endplates of both sides were fractured without involvement of the posterior wall of the vertebral body; this was classified as AOS type A2.

Magnetic resonance imaging and computed tomography after myelography. (A) T2‐weighted magnetic resonance imaging (MRI ) of a sagittal section. (B) Computed tomography (CT ) of a sagittal section after myelography in the supine position revealed that the termination of the spinal cord was at the upper level of the L2 vertebra. (C) This is shown at the white line on CT of an axial section. (B, C) The spinal canal with space around the cord behind the L1 vertebra.

Changes in lateral myelogram views in different positions. Myelogram: (A) Lateral view in flexion position. (B) Lateral view in extension position while lying on the examination table. (C) Lateral view in erect standing position. The dotted white lines show the posterior edge of the vertebrae, and the white arrows indicate the gap of alignment between T12 and L1 in each position. The myelogram depicts the L1 vertebral body protruding into the spinal canal in (C).

Plain postoperative radiographs. Results of postoperative examination with plain radiography: (A) anteroposterior view and (B) lateral view. The alignment of the posterior wall of the vertebrae prevented projection into the spinal canal. Rectangular endcaps were fitted between the inferior T12 and superior L2 endplate.

Computed tomography at 9 months after surgery. (A) Coronal and (B) sagittal sections of computed tomography images at 9 months after surgery. These showed continuity of trabecular bone between cage and endplate without implant failure or cage subsidence.

Schema of the positional relationship between T12 and L1 vertebrae. This figure illustrates the positional relationships between the T12–L2 vertebrae, the posterior longitudinal ligament, and the spinal cord in (A) flexion position, (B) extension position while lying on the examination table, and (C) erect standing position. The white arrow indicates gravitational force. The black arrow shows the direction of T12 downward slippage. The gray arrow shows the backward angulation and “relative retrolisthesis” of L1 into the spinal canal. PLL : Posterior longitudinal ligament.
References
-
- Toda, H. , Okamoto T., Nishida N., Yuba Y., and Iwasaki K.. 2014. Idiopathic hematomyelia as a rare cause of epiconus syndrome. Clin. Neurol. Neurosurg. 125:75–77. - PubMed
-
- Tokuhashi, Y. , Matsuzaki H., Uematsu Y., and Oda H.. 2001. Symptoms of thoracolumbar junction disc herniation. Spine (Phila Pa 1976) 26:E512–E518. - PubMed
-
- Toribatake, Y. , Baba H., Kawahara N., Mizuno K., and Tomita K.. 1997. The epiconus syndrome presenting with radicular‐type neurological features. Spinal Cord 35:163–170. - PubMed
-
- Hashimoto, T. , Kaneda K., and Abumi K.. 1988. Relationship between traumatic spinal canal stenosis and neurologic deficits in thoracolumbar burst fractures. Spine (Phila Pa 1976) 13:1268–1272. - PubMed
-
- Inufusa, A. , An H. S., Lim T. H., Hasegawa T., Haughton V. M., and Nowicki B. H.. 1996. Anatomic changes of the spinal canal and intervertebral foramen associated with flexion‐extension movement. Spine (Phila Pa 1976) 21:2412–2420. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
