

Social Worker-Aided Palliative Care Intervention in High-risk Patients With Heart Failure (SWAP-HF): A Pilot Randomized Clinical Trial
- PMID: 29641819
- PMCID: PMC6128511
- DOI: 10.1001/jamacardio.2018.0589
Social Worker-Aided Palliative Care Intervention in High-risk Patients With Heart Failure (SWAP-HF): A Pilot Randomized Clinical Trial
Abstract
Importance: Palliative care considerations are typically introduced late in the disease trajectory of patients with advanced heart failure (HF), and access to specialty-level palliative care may be limited.
Objective: To determine if early initiation of goals of care conversations by a palliative care-trained social worker would improve prognostic understanding, elicit advanced care preferences, and influence care plans for high-risk patients discharged after HF hospitalization.
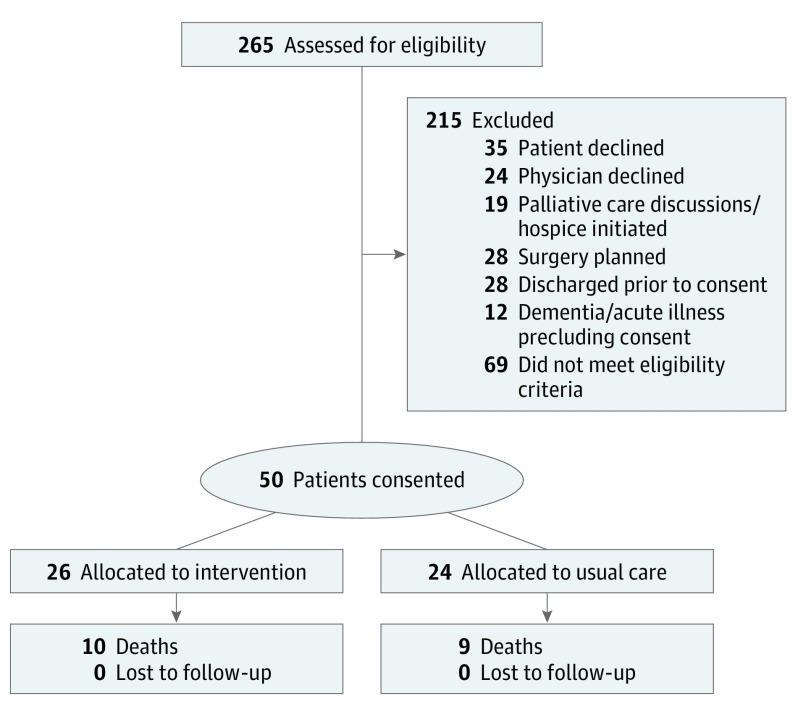
Design, setting, and participants: This prospective, randomized clinical trial of a social worker-led palliative care intervention vs usual care analyzed patients recently hospitalized for management of acute HF who had risk factors for poor prognosis. Analyses were conducted by intention to treat.
Interventions: Key components of the social worker-led intervention included a structured evaluation of prognostic understanding, end-of-life preferences, symptom burden, and quality of life with routine review by a palliative care physician; communication of this information to treating clinicians; and longitudinal follow-up in the ambulatory setting.
Main outcomes and measures: Percentage of patients with physician-level documentation of advanced care preferences and the degree of alignment between patient and cardiologist expectations of prognosis at 6 months.
Results: The study population (N = 50) had a mean (SD) age of 72 (11) years and had a mean (SD) left ventricular ejection fraction of 0.33 (13). Of 50 patients, 41 (82%) had been hospitalized more than once for HF management within 12 months of enrollment. At enrollment, treating physicians anticipated death within a year for 32 patients (64%), but 42 patients (84%) predicted their life expectancy to be longer than 5 years. At 6 months, more patients in the intervention group than in the control group had physician-level documentation of advanced care preferences in the electronic health record (17 [65%] vs 8 [33%]; χ2 = 5.1; P = .02). Surviving patients allocated to intervention were also more likely to revise their baseline prognostic assessment in a direction consistent with the physician's assessment (15 [94%] vs 4 [26%]; χ2 = 14.7; P < .001). Among the 31 survivors at 6 months, there was no measured difference between groups in depression, anxiety, or quality-of-life scores.
Conclusions and relevance: Patients at high risk for mortality from HF frequently overestimate their life expectancy. Without an adverse impact on quality of life, prognostic understanding and patient-physician communication regarding goals of care may be enhanced by a focused, social worker-led palliative care intervention that begins in the hospital and continues in the outpatient setting.
Trial registration: clinicaltrials.gov Identifier: NCT02805712.
Conflict of interest statement
Figures

References
-
- Greener DT, Quill T, Amir O, Szydlowski J, Gramling RE. Palliative care referral among patients hospitalized with advanced heart failure. J Palliat Med. 2014;17(10):1115-1120. - PubMed
-
- Fang JC, Ewald GA, Allen LA, et al. ; Heart Failure Society of America Guidelines Committee . Advanced (stage D) heart failure: a statement from the Heart Failure Society of America Guidelines Committee. J Card Fail. 2015;21(6):519-534. - PubMed
-
- Allen LA, Stevenson LW, Grady KL, et al. ; American Heart Association; Council on Quality of Care and Outcomes Research; Council on Cardiovascular Nursing; Council on Clinical Cardiology; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Surgery and Anesthesia . Decision making in advanced heart failure: a scientific statement from the American Heart Association. Circulation. 2012;125(15):1928-1952. - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
