

Metabolic Syndrome Severity and Risk of CKD and Worsened GFR: The Jackson Heart Study
- PMID: 29642060
- PMCID: PMC6037309
- DOI: 10.1159/000488829
Metabolic Syndrome Severity and Risk of CKD and Worsened GFR: The Jackson Heart Study
Abstract
Background/aims: The metabolic syndrome (MetS), as assessed using dichotomous criteria, is associated with increased risk of future chronic kidney disease (CKD), though this relationship is unclear among African Americans, who have lower risk for MetS but higher risk for CKD.
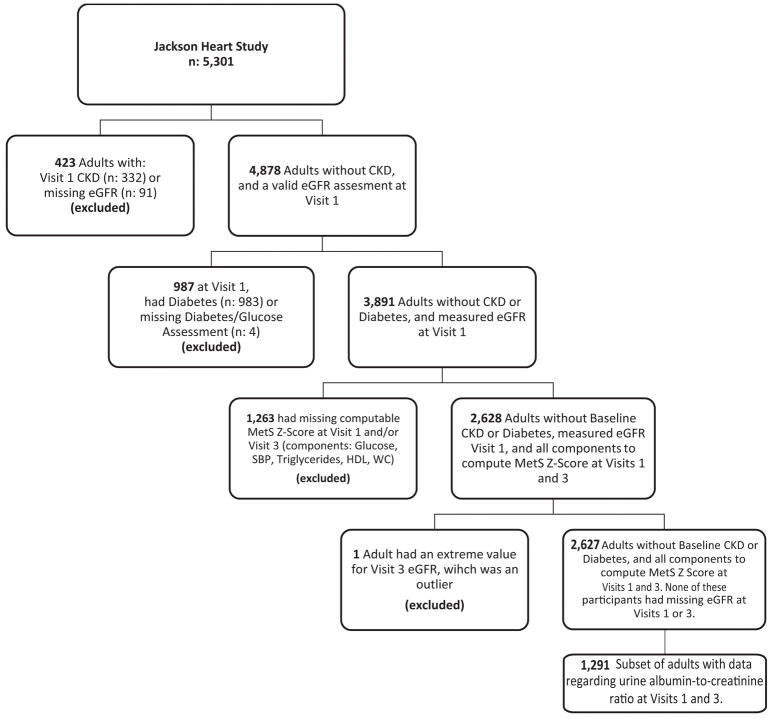
Methods: We performed logistic regression using a sex- and race-specific MetS-severity z-score to assess risk of incident CKD among 2,627 African-American participants of the Jackson Heart Study, assessed at baseline and 8 years later. Based on quartile of baseline MetS severity, we further assessed prevalence of being in the lowest quartile of baseline GFR, the lowest quartile of relative GFR at follow-up, microalbuminuria and incident CKD.
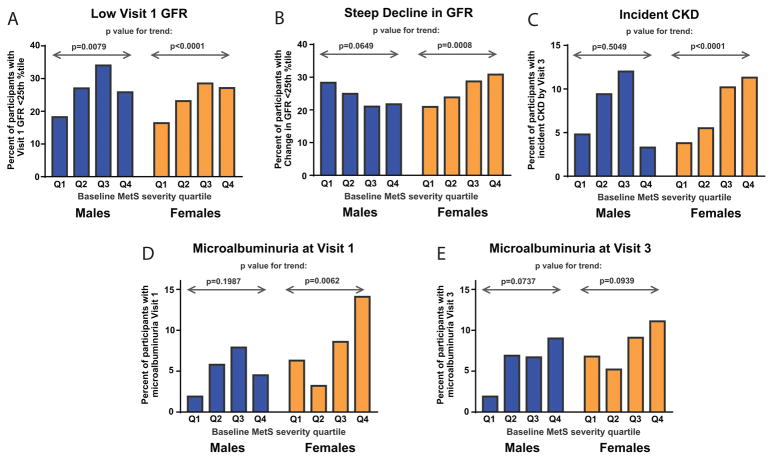
Results: Higher MetS-severity was associated with higher prevalence of GFR in the lowest quartile at baseline among males and females. Among African-American females but not males, higher baseline MetS-severity was associated with a higher prevalence of baseline elevations in microabuminuria (p<0.01), steep decline in GFR (p<0.001) and a higher incidence of CKD (p<0.0001). Women in increasing quartiles of baseline MetS-severity exhibited a linear trend toward higher odds of future CKD (p<0.05), with those in the 4th quartile of MetS-severity (compared to the 1st) having an odds ratio of 2.47 (95% confidence interval 1.13, 5.37); no such relationship was seen among men (p value for trend 0.49).
Conclusion: MetS-severity exhibited sex-based interactions regarding risk for future GFR deterioration and CKD, with increasing risk in women but not men. These data may have implications for triggering CKD screening among African-American women with higher degrees of MetS-severity.
Keywords: Cardiovascular disease; Chronic kidney disease; Glomerular filtration rate; Metabolic syndrome; Microalbuminuria; Risk.
© 2018 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
Figures
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305. - PubMed
-
- Tarver-Carr ME, Powe NR, Eberhardt MS, LaVeist TA, Kington RS, Coresh J, Brancati FL. Excess risk of chronic kidney disease among African-American versus white subjects in the United States: a population-based study of potential explanatory factors. J Am Soc Nephrol. 2002;13:2363–2370. - PubMed
-
- Wong G, Craig JC, Chapman JR. Setting the limit for living kidney donation-how big is too big? Kidney Int. 2017;91:534–536. - PubMed
-
- Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, Gordon DJ, Krauss RM, Savage PJ, Smith SC, Spertus JA, Costa F. Diagnosis and management of the metabolic syndrome - An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112:2735–2752. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
