

Spontaneous conversion of atrial fibrillation caused by severe hyperkalemia: A case report
- PMID: 29642218
- PMCID: PMC5908587
- DOI: 10.1097/MD.0000000000010442
Spontaneous conversion of atrial fibrillation caused by severe hyperkalemia: A case report
Abstract
Rationale: Hyperkalemia is a life-threatening electrolyte disturbance which could lead to arrhythmias and potentially death.
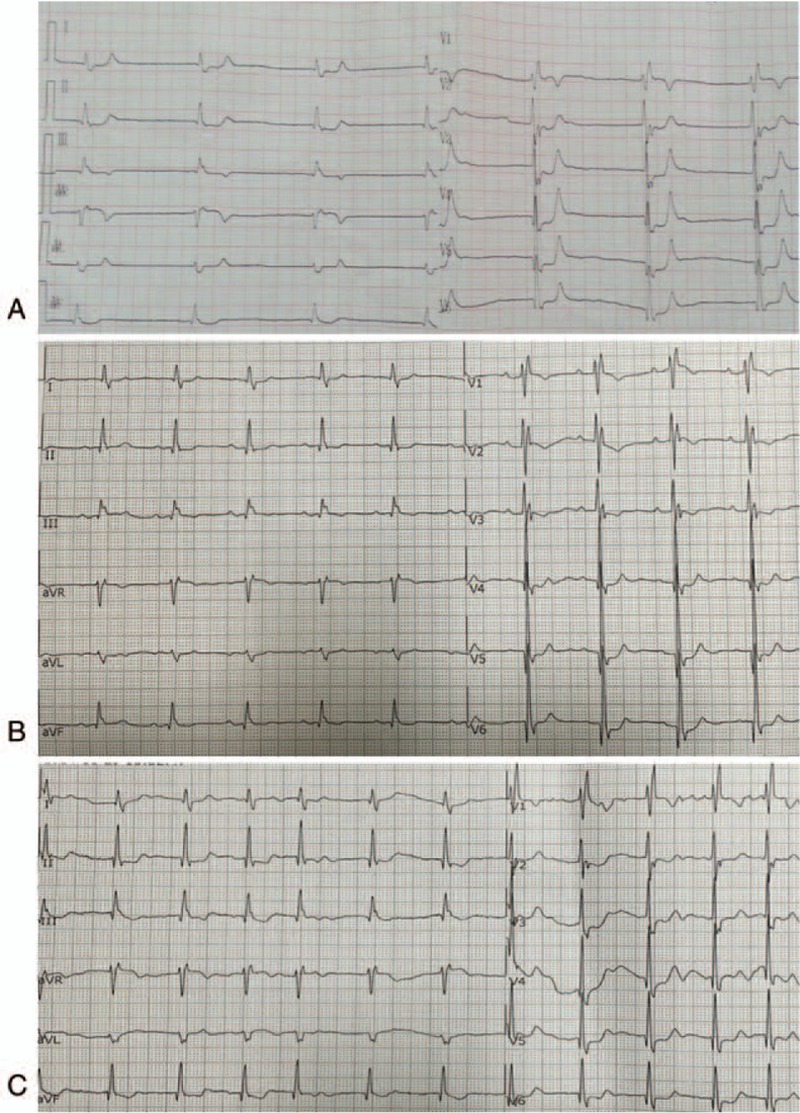
Patient concerns: An 82-year-old male patient who presented typical electrocardiographic indications of hyperkalemia, including the absence of P waves, prolongation of QRS complex, sinoventricular conduction, bradyarrhythmia and tall peaked T waves. He developed a rare self-defibrillation of atrial fibrillation to sinus rhythm due to hyperkalemia. Besides, he developed secondary thrombosis caused by abrupt termination of atrial fibrillation.
Diagnoses: This patient was diagnosed with hyperkalemia, hypertension, and AF.
Interventions: He was treated with an intravenous infusion of calcium gluconate, insulin and dextrose, an oral kayexalate, and emergency hemodialysis.
Outcomes: The patient was managed effectively and discharged with stable status.
Lessons: Hyperkalemia could induce malignant arrhythmia with high mortality. Thus we suggested more attention be paid to monitoring electrolyte disorders and maintaining anticoagulation treatments to avoid thromboembolism.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
Hyperkalemia-induced conversion of permanent atrial fibrillation to normal sinus rhythm: a case report.J Cardiovasc Med (Hagerstown). 2011 Sep;12(9):678-80. doi: 10.2459/JCM.0b013e32833ce871. J Cardiovasc Med (Hagerstown). 2011. PMID: 20671568 No abstract available.
-
Tako-Tsubo cardiomyopathy and spontaneous cardioversion of permanent atrial fibrillation associated with acute hyperkalemia.Int J Cardiol. 2013 Aug 10;167(3):e67-70. doi: 10.1016/j.ijcard.2013.03.117. Epub 2013 Apr 17. Int J Cardiol. 2013. PMID: 23602299 No abstract available.
-
Electrocardiographic manifestations of hyperkalemia.Am J Emerg Med. 2000 Oct;18(6):721-9. doi: 10.1053/ajem.2000.7344. Am J Emerg Med. 2000. PMID: 11043630
-
Electrocardiographic manifestations of severe hyperkalemia.J Electrocardiol. 2018 Sep-Oct;51(5):814-817. doi: 10.1016/j.jelectrocard.2018.06.018. Epub 2018 Jul 4. J Electrocardiol. 2018. PMID: 30177318 Review.
-
Management of severe hyperkalemia without hemodialysis: case report and literature review.J Crit Care. 2006 Dec;21(4):316-21. doi: 10.1016/j.jcrc.2005.10.001. J Crit Care. 2006. PMID: 17175417 Review.
Cited by
-
ECG alterations suggestive of hyperkalemia in normokalemic versus hyperkalemic patients.BMC Emerg Med. 2019 May 31;19(1):33. doi: 10.1186/s12873-019-0247-0. BMC Emerg Med. 2019. PMID: 31151388 Free PMC article.
-
Cardioversion à la carte - your choice of the unconventional.Oxf Med Case Reports. 2024 Jan 27;2024(1):omae002. doi: 10.1093/omcr/omae002. eCollection 2024 Jan. Oxf Med Case Reports. 2024. PMID: 38292161 Free PMC article. No abstract available.
-
Clinical and electrocardiogram presentations of patients with high serum potassium concentrations within emergency settings: a prospective study.Int J Emerg Med. 2022 May 26;15(1):23. doi: 10.1186/s12245-022-00422-8. Int J Emerg Med. 2022. PMID: 35619089 Free PMC article.
-
Artificial Intelligence-Driven Algorithm for Drug Effect Prediction on Atrial Fibrillation: An in silico Population of Models Approach.Front Physiol. 2021 Dec 6;12:768468. doi: 10.3389/fphys.2021.768468. eCollection 2021. Front Physiol. 2021. PMID: 34938202 Free PMC article.
References
-
- Oh PC, Koh KK, Kim JH, et al. Life threatening severe hyperkalemia presenting typical electrocardiographic changes-rapid recovery following medical, temporary pacing, and hemodialysis treatments. Int J Cardiol 2014;177:27–9. - PubMed
-
- Sood MM, Sood AR, Richardson R. Emergency management and commonly encountered outpatient scenarios in patients with hyperkalemia. Mayo Clin Proc 2007;82:1553–61. - PubMed
-
- Cohen E, Nardi Y, Krause I, et al. A longitudinal assessment of the natural rate of decline in renal function with age. J Nephrol 2014;27:635–41. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
