

Assessing the healthcare resource use associated with inappropriate prescribing of inhaled corticosteroids for people with chronic obstructive pulmonary disease (COPD) in GOLD groups A or B: an observational study using the Clinical Practice Research Datalink (CPRD)
- PMID: 29642882
- PMCID: PMC5896104
- DOI: 10.1186/s12931-018-0767-2
Assessing the healthcare resource use associated with inappropriate prescribing of inhaled corticosteroids for people with chronic obstructive pulmonary disease (COPD) in GOLD groups A or B: an observational study using the Clinical Practice Research Datalink (CPRD)
Abstract
Background: Recent recommendations from the Global Initiative for Chronic Obstructive Lung Disease (GOLD) position inhaled corticosteroids (ICS) for use in chronic obstructive pulmonary disease (COPD) patients experiencing exacerbations (≥ 2 or ≥ 1 requiring hospitalisation); i.e. GOLD groups C and D. However, it is known that ICS is frequently prescribed for patients with less severe COPD. Potential drivers of inappropriate ICS use may be historical clinical guidance or a belief among physicians that intervening early with ICS would improve outcomes and reduce resource use. The objective of this study was to compare healthcare resource use in the UK for COPD patients in GOLD groups A and B (0 or 1 exacerbation not resulting in hospitalisation) who have either been prescribed an ICS-containing regimen or a non-ICS-containing regimen.
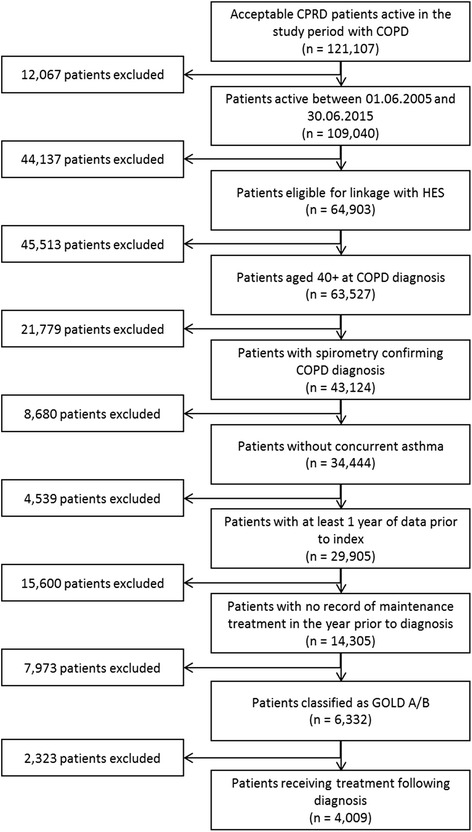
Methods: Linked data from the Clinical Practice Research Datalink (CPRD) and Hospital Episode Statistics (HES) database were used. For the study period (1 July 2005 to 30 June 2015) a total 4009 patients met the inclusion criteria; 1745 receiving ICS-containing therapy and 2264 receiving non-ICS therapy. Treatment groups were propensity score-matched to account for potential confounders in the decision to prescribe ICS, leaving 1739 patients in both treatment arms. Resource use was assessed in terms of frequency of healthcare practitioner (HCP) interactions and rescue therapy prescribing. Treatment acquisition costs were not assessed.
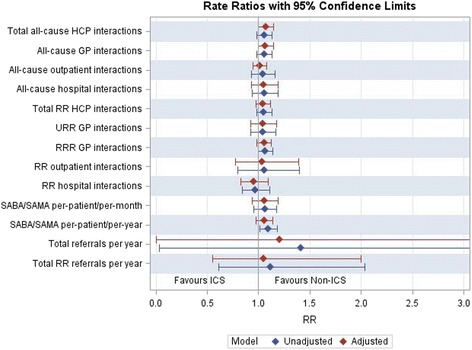
Results: Results showed no benefit associated with the addition of ICS, with numerically higher all-cause HCP interactions (72,802 versus 69,136; adjusted relative rate: 1.07 [p = 0.061]) and rescue therapy prescriptions (24,063 versus 21,163; adjusted relative rate: 1.05 [p = 0.212]) for the ICS-containing group compared to the non-ICS group. Rate ratios favoured the non-ICS group for eight of nine outcomes assessed. Outcomes were similar for subgroup analyses surrounding potential influential parameters, including patients with poorer lung function (FEV1 < 50% predicted), one prior exacerbation or elevated blood eosinophils.
Conclusions: These data suggest that ICS use in GOLD A and B COPD patients is not associated with a benefit in terms of healthcare resource use compared to non-ICS bronchodilator-based therapy; using ICS according to GOLD recommendations may offer an opportunity for improving patient care and reducing resource use.
Keywords: Chronic obstructive pulmonary disease; Inhaled corticosteroids, Long-acting bronchodilators; Resource use.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval was obtained from ISAC (the Independent Scientific Advisory Committee overseeing CPRD), protocol 16_173R.
Linked pseudonymised data was provided for this study by CPRD. Data is linked by NHS Digital, the statutory trusted third party for linking data, using identifiable data held only by NHS Digital. Select general practices consent to this process at a practice level with individual patients having the right to opt-out.
Competing interests
JC has received research grants from Boehringer Ingelheim, AstraZeneca, GlaxoSmithKline and Pfizer. JC has also received fees for consultancy and speaking from Boehringer Ingelheim.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Snell N, Strachan D, Hubbard R, Gibson J, Gruffydd-Jones K, Jarrold I. S32 Epidemiology of chronic obstructive pulmonary disease (COPD) in the uk: findings from the british lung foundation’s ‘respiratory health of the nation’ project. Thorax. 2016;71(Suppl 3):A20-A.
-
- Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi: 10.1164/rccm.201701-0218PP. - DOI - PubMed
-
- Jones R, Freemantle N, Miravitlles M, Bruselle G, Gruffydd-Jones K, Baldwin M, et al. Inappropriate prescriptions following initial COPD diagnosis. Eur Respir J. 2013;42(Suppl 57):2391.
-
- Vogelmeier CF, Bateman ED, Pallante J, Alagappan VK, D'Andrea P, Chen H, et al. Efficacy and safety of once-daily QVA149 compared with twice-daily salmeterol-fluticasone in patients with chronic obstructive pulmonary disease (ILLUMINATE): a randomised, double-blind, parallel group study. Lancet Respir Med. 2013;(1, 1):51–60. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
