

Reverse shock index multiplied by Glasgow Coma Scale score (rSIG) is a simple measure with high discriminant ability for mortality risk in trauma patients: an analysis of the Japan Trauma Data Bank
- PMID: 29642920
- PMCID: PMC5896075
- DOI: 10.1186/s13054-018-2014-0
Reverse shock index multiplied by Glasgow Coma Scale score (rSIG) is a simple measure with high discriminant ability for mortality risk in trauma patients: an analysis of the Japan Trauma Data Bank
Abstract
Background: The shock index (SI), defined as heart rate (HR) divided by systolic blood pressure (SBP), is reported to be a more sensitive marker of shock than traditional vital signs alone. In previous literature, use of the reverse shock index (rSI), taken as SBP divided by HR, is recommended instead of SI for hospital triage. Among traumatized patients aged > 55 years, SI multiplied by age (SIA) might provide better prediction of early post-injury mortality. Separately, the Glasgow Coma Scale (GCS) score has been shown to be a very strong predictor. When considering these points together, rSI multiplied by GCS score (rSIG) or rSIG divided by age (rSIG/A) could provide even better prediction of in-hospital mortality.
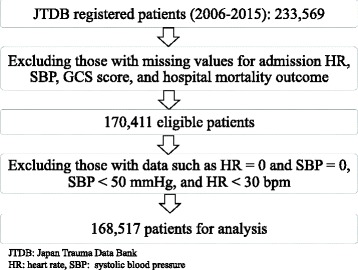
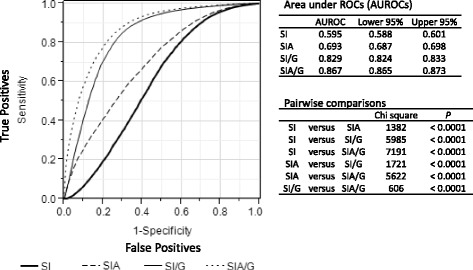
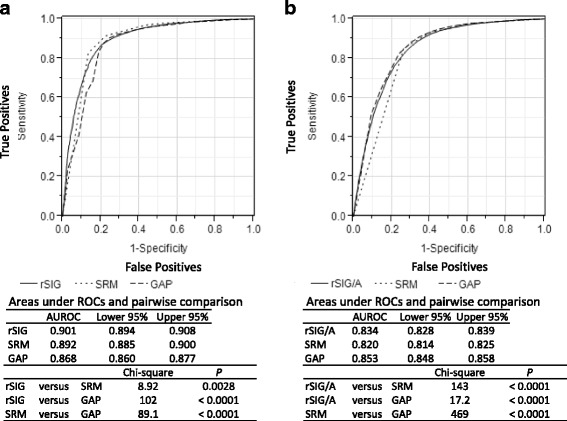
Methods: This retrospective, multicenter study used data from 168,517 patients registered in the Japan Trauma Data Bank for the period 2006-2015. We calculated areas under receiver operating characteristic curves (AUROCs) to measure the discriminant ability by comparing those of SI (or rSI), SIA, rSIG, and rSIG/A for in-hospital mortality and for 24-h blood transfusion.
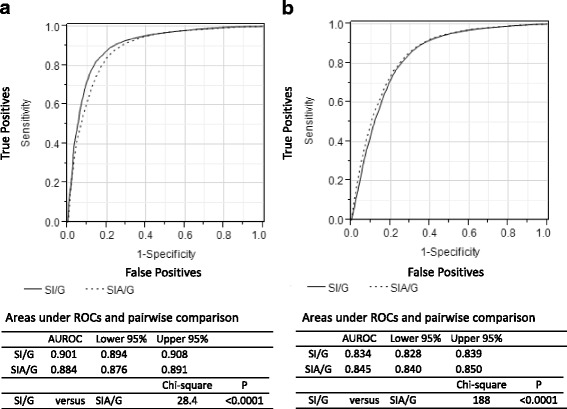
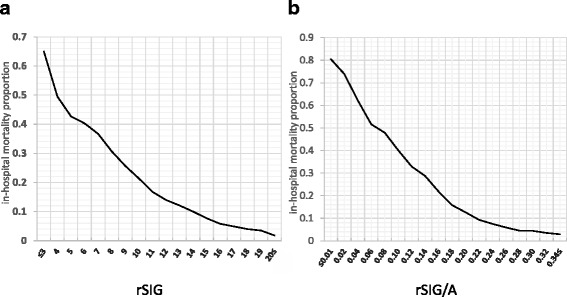
Results: The highest ROC AUC (AUROC), 0.901(0.894-0.908) for in-hospital mortality in younger patients (aged < 55 years), was seen for rSIG. In older patients (aged ≥ 55 years), the AUROC of rSIG/A, 0.845(0.840-0.850), was highest for in-hospital mortality. However, the difference between rSIG and rSIG/A was slight and did not seem to be clinically important. rSIG also had the highest AUROC of 0.745 (0.741-749) for 24-h blood transfusion.
Conclusions: rSIG ((SBP/HR) × GCS score) is easy to calculate without the need for additional information, charts or equipment, and can be a more reliable triage tool for identifying risk levels in trauma patients.
Keywords: Glasgow Coma Scale score; Heart rate; In-hospital mortality; Japan Trauma Data Bank; Systolic blood pressure.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the research ethics committee of the National Center for Global Health and Medicine (NCGM-G-001863-00), which waived the requirement for informed consent from patients because of the anonymous nature of the data.
Consent for publication
We have provided information about the implementation of the trauma registry (JTDB) and the utilization of it for scientific researches by a poster at our hospital and by the website of our emergency department.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Mutschler M, Nienaber U, Münzberg M, Wölfl C, Schoechl H, PaffrathT BB, Maegele M, the TraumaRegister DGU ®. The Shock Index revisited – a fast guide to transfusion requirement? A retrospective analysis on 21,853 patients derived from the TraumaRegister DGU ®. Crit Care. 2013;17:R172. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
