

Diagnostic and management of life-threatening Adult-Onset Still Disease: a French nationwide multicenter study and systematic literature review
- PMID: 29642928
- PMCID: PMC5896069
- DOI: 10.1186/s13054-018-2012-2
Diagnostic and management of life-threatening Adult-Onset Still Disease: a French nationwide multicenter study and systematic literature review
Abstract
Background: Adult-onset Still disease (AOSD) is a rare systemic inflammatory disorder. A few patients develop organ complications that can be life-threatening. Our objectives were to describe the disease course and phenotype of life-threatening AOSD, including response to therapy and long-term outcome.
Methods: A multicenter case series of intensive care medicine (ICU) patients with life-threatening AOSD and a systematic literature review.
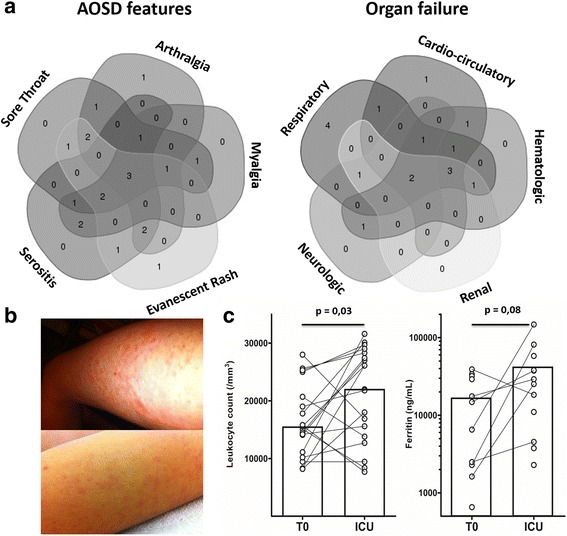
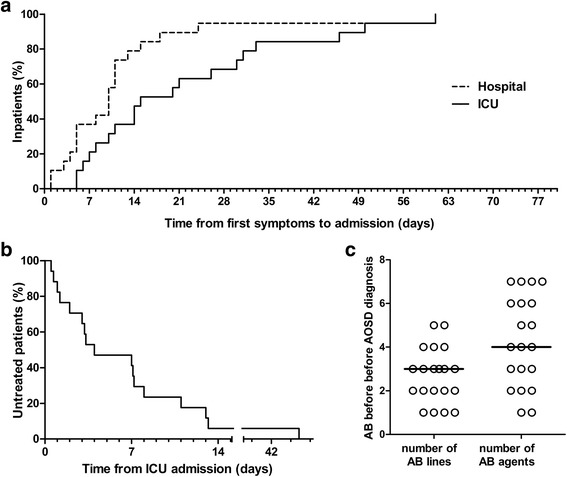
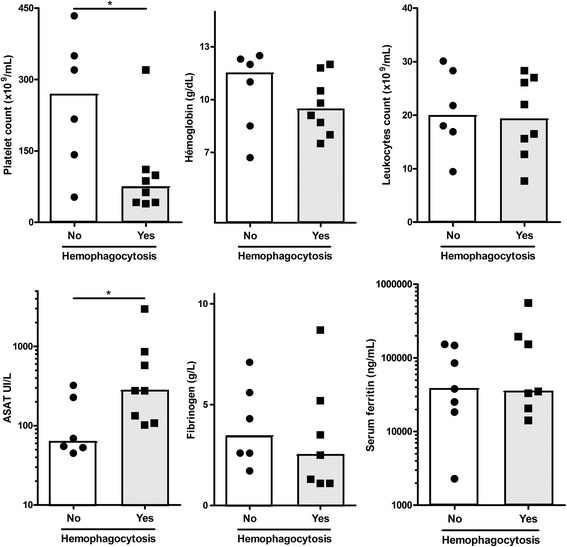
Results: Twenty patients were included. ICU admission mostly occurred at disease onset (90%). Disease manifestations included fever (100%), sore throat (65%), skin rash (65%), and arthromyalgia (55%). Serum ferritin was markedly high (median: 29,110 ng/mL). Acute respiratory failure, shock and multiple organ failure occurred in 15 (75%), 10 (50%), and 7 (35%) cases, respectively. Hemophagocytosis was demonstrated in eight cases. Two patients died. Treatment delay was significant. All patients received corticosteroids. Response rate was 50%. As second-line, intravenous immunoglobulins were ineffective. Anakinra was highly effective. After ICU discharge, most patients required additional treatment. Literature analysis included 79 cases of AOSD with organ manifestations, which mainly included reactive hemophagocytic syndrome (42%), acute respiratory failure (34%), and cardiac complications (23%). Response rate to corticosteroids was 68%. Response rates to IVIgs, cyclosporin, and anakinra were 50%, 80%, and 100%, respectively.
Conclusions: AOSD should be recognized as a rare cause of sepsis mimic in patients with fever of unknown origin admitted to the ICU. The diagnosis relies on a few simple clinical clues. Early intensive treatment may be discussed. IVIgs should be abandoned. Long-term prognosis is favorable.
Keywords: Adult onset Still disease; Anakinra; Cyclosporin; Differential diagnosis; ICU; Intravenous immunoglobulins; Reactive hemophagocytic syndrome; Shock.
Conflict of interest statement
Ethics approval and consent to participate
This observational study was performed in accordance with the Helsinki declaration, European and French ethical laws.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
