

Findings of the Chronic Obstructive Pulmonary Disease-Sitting and Exacerbations Trial (COPD-SEAT) in Reducing Sedentary Time Using Wearable and Mobile Technologies With Educational Support: Randomized Controlled Feasibility Trial
- PMID: 29643055
- PMCID: PMC5917078
- DOI: 10.2196/mhealth.9398
Findings of the Chronic Obstructive Pulmonary Disease-Sitting and Exacerbations Trial (COPD-SEAT) in Reducing Sedentary Time Using Wearable and Mobile Technologies With Educational Support: Randomized Controlled Feasibility Trial
Abstract
Background: Targeting sedentary time post exacerbation may be more relevant than targeting structured exercise for individuals with chronic obstructive pulmonary disease. Focusing interventions on sitting less and moving more after an exacerbation may act as a stepping stone to increase uptake to pulmonary rehabilitation.
Objective: The aim of this paper was to conduct a randomized trial examining trial feasibility and the acceptability of an education and self-monitoring intervention using wearable technology to reduce sedentary behavior for individuals with chronic obstructive pulmonary disease admitted to hospital for an acute exacerbation.
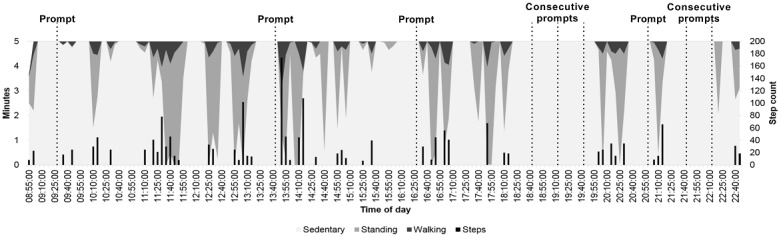
Methods: Participants were recruited and randomized in hospital into 3 groups, with the intervention lasting 2 weeks post discharge. The Education group received verbal and written information about reducing their time in sedentary behavior, sitting face-to-face with a study researcher. The Education+Feedback group received the same education component along with real-time feedback on their sitting time, stand-ups, and steps at home through a waist-worn inclinometer linked to an app. Patients were shown how to use the technology by the same study researcher. The inclinometer also provided vibration prompts to encourage movement at patient-defined intervals of time. Patients and health care professionals involved in chronic obstructive pulmonary disease exacerbation care were interviewed to investigate trial feasibility and acceptability of trial design and methods. Main quantitative outcomes of trial feasibility were eligibility, uptake, and retention, and for acceptability, were behavioral responses to the vibration prompts.
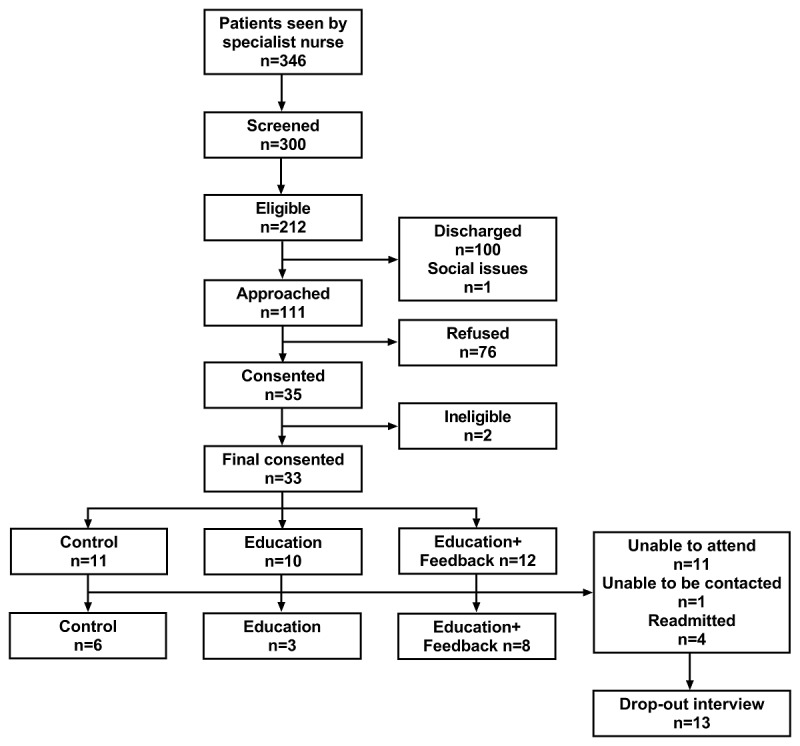
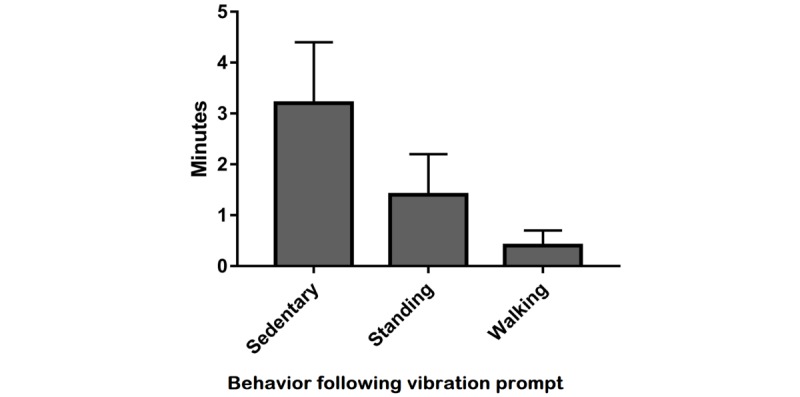
Results: In total, 111 patients were approached with 33 patients recruited (11 Control, 10 Education, and 12 Education+Feedback). Retention at 2-week follow-up was 52% (17/33; n=6 for Control, n=3 for Education, and n=8 for Education+Feedback). No study-related adverse events occurred. Collectively, patients responded to 106 out of 325 vibration prompts from the waist-worn inclinometer (32.62%). Within 5 min of the prompt, 41% of responses occurred, with patients standing for a mean 1.4 (SD 0.8) min and walking for 0.4 (SD 0.3) min (21, SD 11, steps). Interviews indicated that being unwell and overwhelmed after an exacerbation was the main reason for not engaging with the intervention. Health care staff considered reducing sedentary behavior potentially attractive for patients but suggested starting the intervention as an inpatient.
Conclusions: Although the data support that it was feasible to conduct the trial, modifications are needed to improve participant retention. The intervention was acceptable to most patients and health care professionals.
Trial registration: International Standard Randomized Controlled Trial Number (ISRCTN) 13790881; http://www.isrctn.com/ISRCTN13790881 (Archived by WebCite at http://www.webcitation.org/6xmnRGjFf).
Keywords: chronic obstructive pulmonary disease; feasibility; fitness trackers; intervention; physical activity; sedentary lifestyle; sedentary time; self-monitoring; wearable electronic devices.
©Mark W Orme, Amie E Weedon, Paula M Saukko, Dale W Esliger, Mike D Morgan, Michael C Steiner, John W Downey, Lauren B Sherar, Sally J Singh. Originally published in JMIR Mhealth and Uhealth (http://mhealth.jmir.org), 11.04.2018.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Burge S, Wedzicha JA. COPD exacerbations: definitions and classifications. Eur Respir J Suppl. 2003 Jun;41:46s–53s. http://erj.ersjournals.com/cgi/pmidlookup?view=long&pmid=12795331 - PubMed
-
- Jones SE, Green SA, Clark AL, Dickson MJ, Nolan AM, Moloney C, Kon SS, Kamal F, Godden J, Howe C, Bell D, Fleming S, Haselden BM, Man WD. Pulmonary rehabilitation following hospitalisation for acute exacerbation of COPD: referrals, uptake and adherence. Thorax. 2014 Feb;69(2):181–2. doi: 10.1136/thoraxjnl-2013-204227.thoraxjnl-2013-204227 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
