

A novel two-score system for interferon status segregates autoimmune diseases and correlates with clinical features
- PMID: 29643425
- PMCID: PMC5895784
- DOI: 10.1038/s41598-018-24198-1
A novel two-score system for interferon status segregates autoimmune diseases and correlates with clinical features
Erratum in
-
Publisher Correction: A novel two-score system for interferon status segregates autoimmune diseases and correlates with clinical features.Sci Rep. 2018 Oct 1;8(1):14846. doi: 10.1038/s41598-018-33062-1. Sci Rep. 2018. PMID: 30275491 Free PMC article.
Abstract
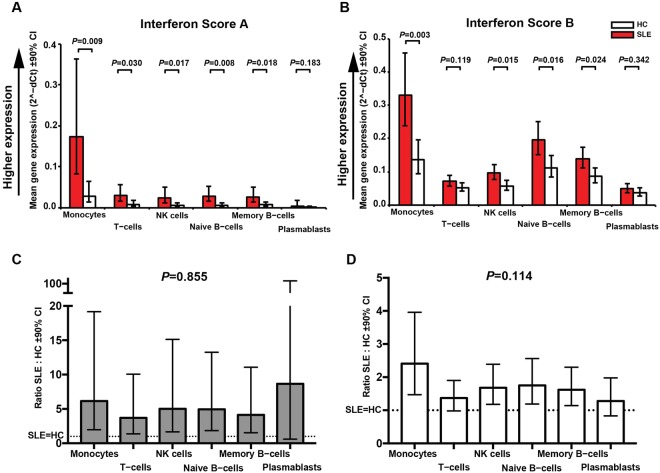
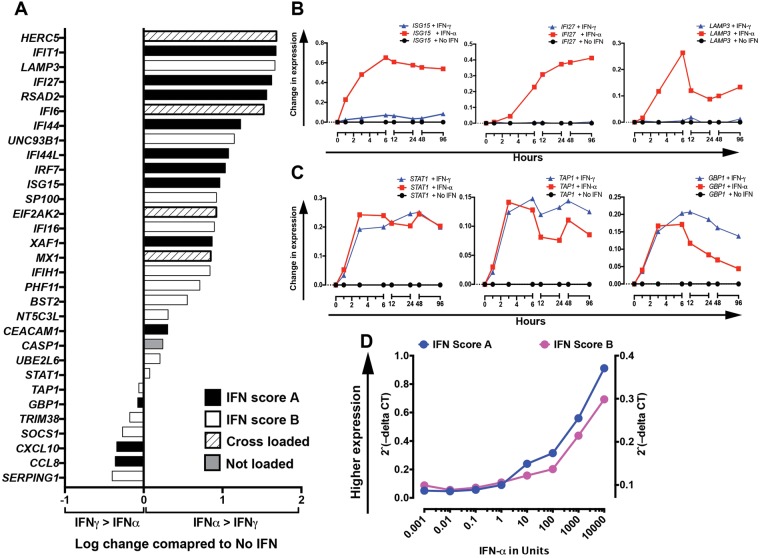
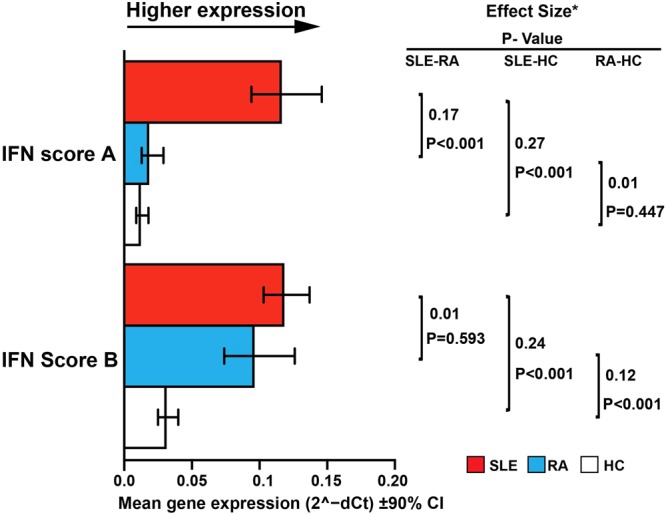
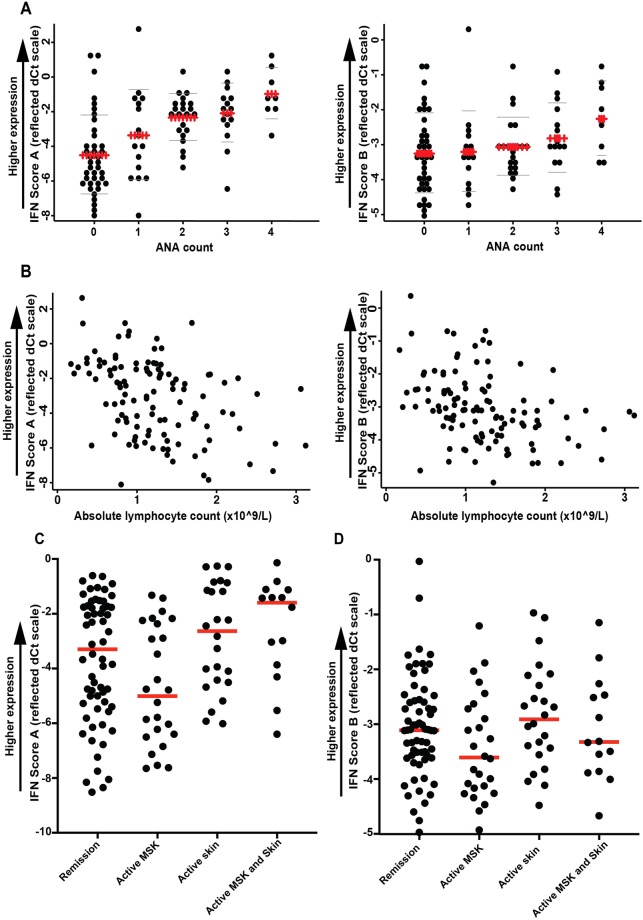
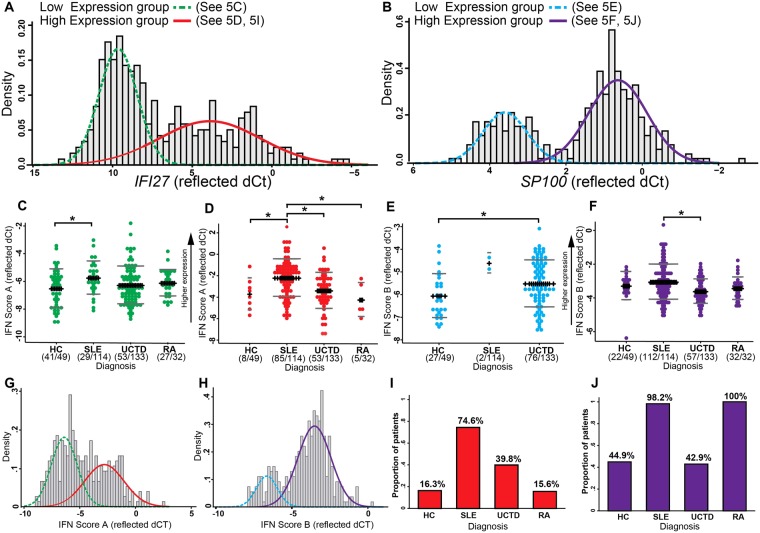
Measurement of type I interferon (IFN-I) has potential to diagnose and stratify autoimmune diseases, but existing results have been inconsistent. Interferon-stimulated-gene (ISG) based methods may be affected by the modularity of the ISG transcriptome, cell-specific expression, response to IFN-subtypes and bimodality of expression. We developed and clinically validated a 2-score system (IFN-Score-A and -B) using Factor Analysis of 31 ISGs measured by TaqMan selected from 3-IFN-annotated modules. We evaluated these scores using in-vitro IFN stimulation as well as in sorted cells then clinically validated in a cohort of 328 autoimmune disease patients and healthy controls. ISGs varied in response to IFN-subtypes and both scores varied between cell subsets. IFN-Score-A differentiated Systemic Lupus Erythematosus (SLE) from both Rheumatoid Arthritis (RA) and Healthy Controls (HC) (both p < 0.001), while IFN-Score-B differentiated SLE and RA from HC (both p < 0.001). In SLE, both scores were associated with cutaneous and hematological (all p < 0.05) but not musculoskeletal disease activity. Comparing with bimodal (IFN-high/low) classification, significant differences in IFN-scores were found between diagnostic groups within the IFN-high group. Our continuous 2-score system is more clinically relevant than a simple bimodal classification of IFN status. This system should allow improvement in diagnosis, stratification, and therapy in IFN-mediated autoimmunity.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Psarras, A., Emery, P. & Vital, E. M. Type I interferon-mediated autoimmune diseases: pathogenesis, diagnosis and targeted therapy. Rheumatology (Oxford), 10.1093/rheumatology/kew431 (2017). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
