

Cost-effectiveness of the recommended medical intervention for the treatment of dysmenorrhea and endometriosis in Japan
- PMID: 29643744
- PMCID: PMC5891893
- DOI: 10.1186/s12962-018-0097-8
Cost-effectiveness of the recommended medical intervention for the treatment of dysmenorrhea and endometriosis in Japan
Abstract
Background and objective: This study aims to assess the cost-effectiveness of early physician consultation and guideline-based intervention to prevent endometriosis and/or disease progression using oral contraceptive (OC) and progestin compared to follow-up of self-care for dysmenorrhea in Japan.
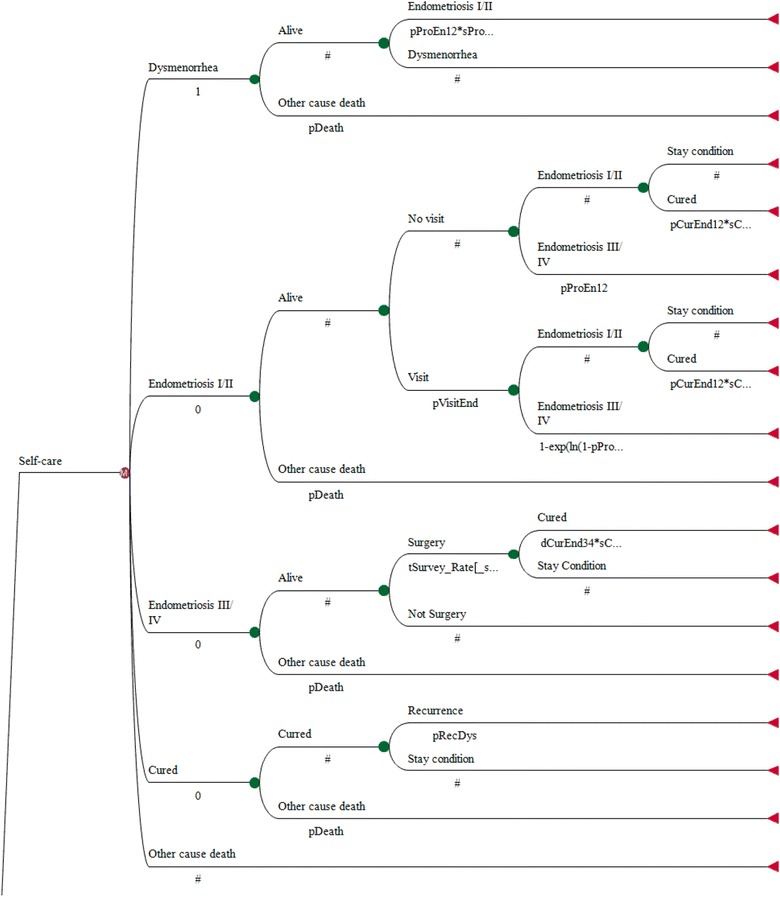
Methods: A yearly-transmitted Markov model of five major health states with four sub-medical states was constructed. Transition probabilities among health and medical states were derived from Japanese epidemiological patient surveys and converted to appropriate parameters for inputting into the model. The dysmenorrhea and endometriosis-associated direct costs included inpatient, outpatient visit, surgery, and medication (OC agents, over-the-counter drugs), etc. The utility measure for patients with phase I-IV endometriosis comprised a visual analogue scale. We estimated the cost per quality-adjusted life year (QALY) at a time horizon of 23 years. An annual discount rate at 3% for both cost and outcome was considered.
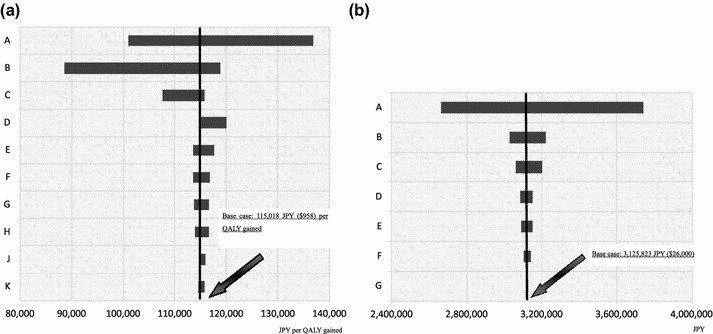
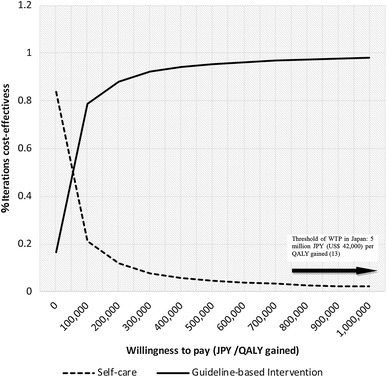
Results: The base case outcomes indicated that the intervention would be more cost-effective than self-care, as the incremental cost-effectiveness ratio (ICER) yielded 115,000 JPY per QALY gained from the healthcare payers' perspective and the societal monetary value (SMV) was approximately positive 3,130,000 JPY, favoring the intervention in the cost-benefit estimate. A tornado diagram depicting the stochastic sensitivity analysis of the ICER and SMV from both the healthcare payers' and societal perspectives confirmed the robustness of the base case. A probabilistic analysis resulting from 10,000-time Monte Carlo simulations demonstrated efficiency at willingness-to-pay thresholds in more than 90% of the iterations.
Conclusions: The present analysis demonstrated that early physician consultation and guideline-based intervention would be more cost-effective than self-care in preventing endometriosis and/or disease progression for patients with dysmenorrhea in Japan.
Keywords: Cost-effectiveness; Dysmenorrhea; Endometriosis; Guideline-based intervention; Self-care.
Figures
References
-
- Taketani Y, Ishimaru T, Hoshiai H, et al. Research on current situation and treatment strategies of endometriosis from viewpoint of reproductive health. Health Sciences Research Grant-in-Aid in 1997. 1998. p. 99–104. https://www.niph.go.jp/wadai/mhlw/ssh_1997_16.htm. Accessed 13 July 2016. (in Japanese).
-
- Guideline on treatment in obstetrics and gynecology. Outpatient visit version 2014. http://www.jsog.or.jp/activity/pdf/gl_fujinka_2014.pdf. Accessed 30 Aug 2016.
LinkOut - more resources
Full Text Sources
Other Literature Sources
