

Interstitial inflammation and interstitial fibrosis and tubular atrophy predict renal survival in lupus nephritis
- PMID: 29644061
- PMCID: PMC5888814
- DOI: 10.1093/ckj/sfx093
Interstitial inflammation and interstitial fibrosis and tubular atrophy predict renal survival in lupus nephritis
Abstract
Background: This study examines the effect of interstitial inflammation and interstitial fibrosis and tubular atrophy on renal survival in lupus nephritis.
Methods: Baseline characteristics, initial (n = 301) and repeat biopsies (n = 94) and clinical outcomes for patients with biopsy-proven lupus nephritis from 1998 to 2014 were retrospectively collected from the medical record. Clinical and morphologic variables were evaluated using a Cox proportional hazards model and multiple imputation to address missing data. Renal survival was defined as the time from initial biopsy to end-stage renal disease [estimated glomerular filtration rate (eGFR) <15 mL/min/1.73 m2], dialysis or transplant.
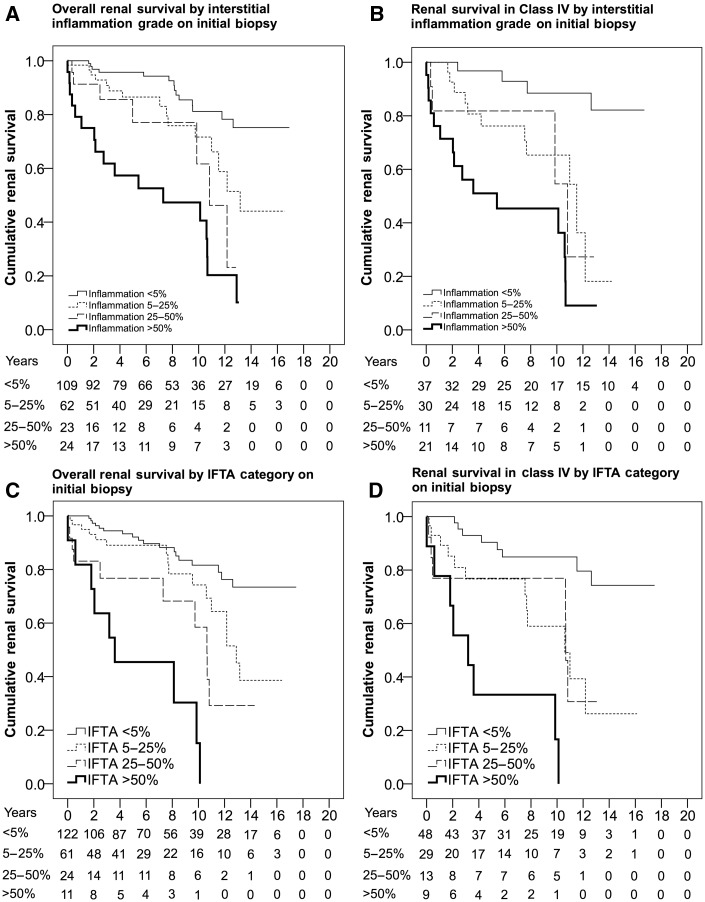
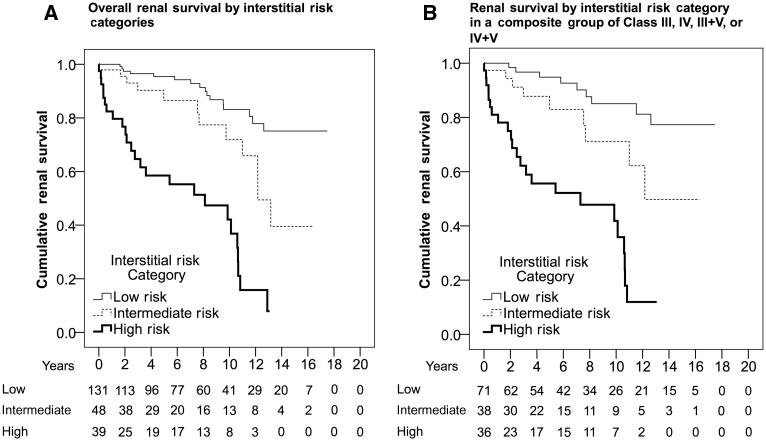
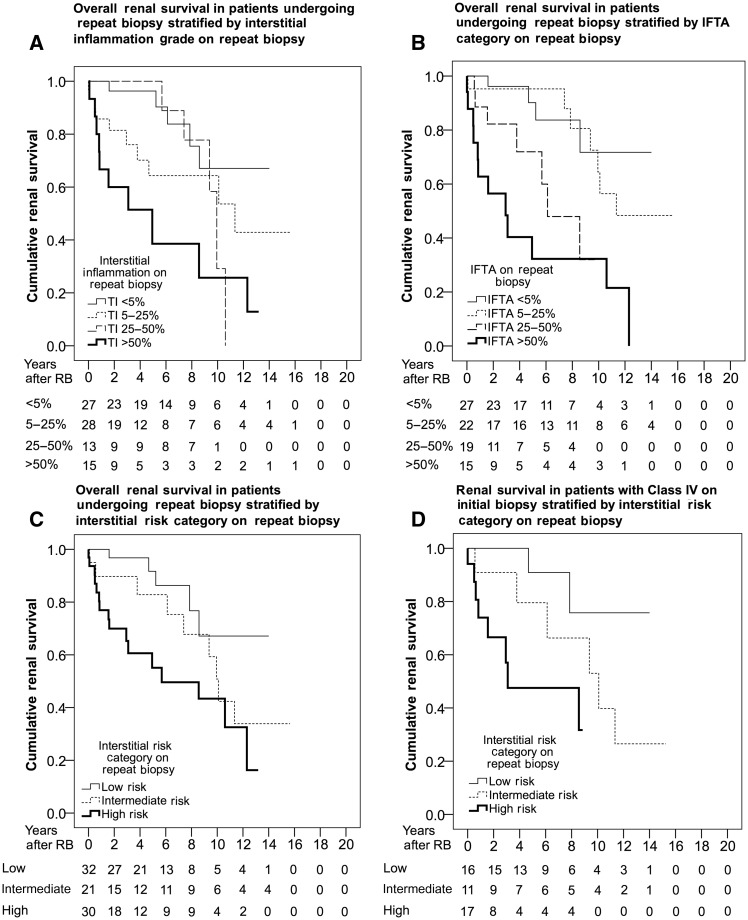
Results: A total of 218 patients had follow-up and Class IV had worse renal survival, especially in patients with active and chronic glomerular lesions {relative to non-IV; Class IV-A: hazard ratio [HR] 0.92 [95% confidence interval (CI) 0.41-2.04], Class IV-AC: HR 5.02 [95% CI 2.70-9.36]}. Interstitial inflammation grade [relative to interstitial inflammation <5%; interstitial inflammation 5-25%: HR 2.36 (95% CI 1.13-4.91), interstitial inflammation 25-50%: HR 3.84 (95% CI 1.53-9.62), interstitial inflammation >50%: HR 7.67 (95% CI 3.75-15.67)] and increased interstitial fibrosis and tubular atrophy (IFTA) category [relative to IFTA <5%; IFTA 5-25%: HR 3.93 (95% CI 1.58-9.75), IFTA 25-50%: HR 4.01 (95% CI 1.37-11.70), IFTA >50%: HR 13.99 (95% CI 4.91-39.83)] predicted worse renal survival among all patients and those with Class IV on initial and repeat biopsy (n = 94) in a dose-dependent manner. Interstitial inflammation grade and IFTA category were significant predictors of renal survival in a multivariable model adjusted for age, gender, race, ethnicity and serum creatinine.
Conclusions: Interstitial inflammation and IFTA independently affect renal survival and grading these lesions stratifies risk within the International Society of Nephrology and Renal Pathology Society classification of lupus nephritis.
Keywords: interstitial fibrosis; interstitial inflammation; kidney biopsy; lupus nephritis; renal pathology; tubular atrophy.
Figures

References
-
- Korbet SM, Schwartz MM, Evans J. et al. Severe lupus nephritis: racial differences in presentation and outcome. J Am Soc Nephrol 2007; 18: 244–254 - PubMed
-
- Nee R, Martinez-Osorio J, Yuan CM. et al. Survival disparity of African-American versus non-African-American patients with ESRD due to SLE. Am J Kidney Dis 2015; 66: 630–637 - PubMed
-
- Weening JJ, D'Agati VD, Schwartz MM. et al. The classification of glomerulonephritis in systemic lupus erythematosus revisited. J Am Soc Nephrol 2004; 15: 241–250 - PubMed
-
- Wilhelmus S, Bajema IM, Bertsias GK. et al. Lupus nephritis management guidelines compared. Nephrol Dial Transplant 2016; 31: 904–913 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
