

Femoral neck pseudoarthrosis in a polio patient treated with closed reduction and cell therapy
- PMID: 29644312
- PMCID: PMC5883191
- DOI: 10.1016/j.tcr.2017.01.018
Femoral neck pseudoarthrosis in a polio patient treated with closed reduction and cell therapy
Abstract
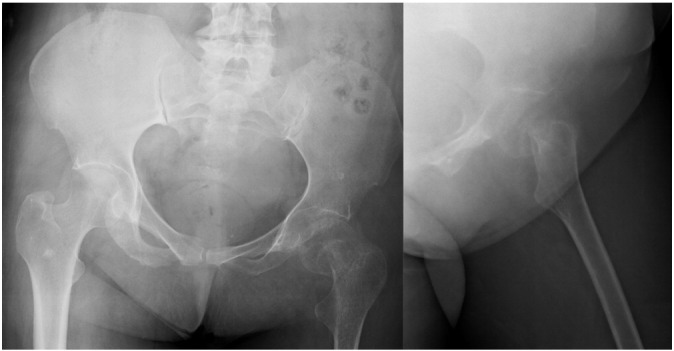
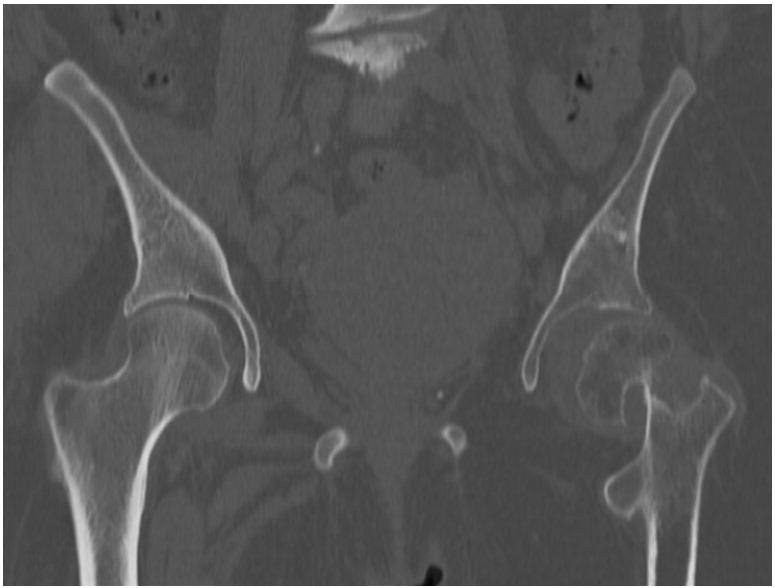
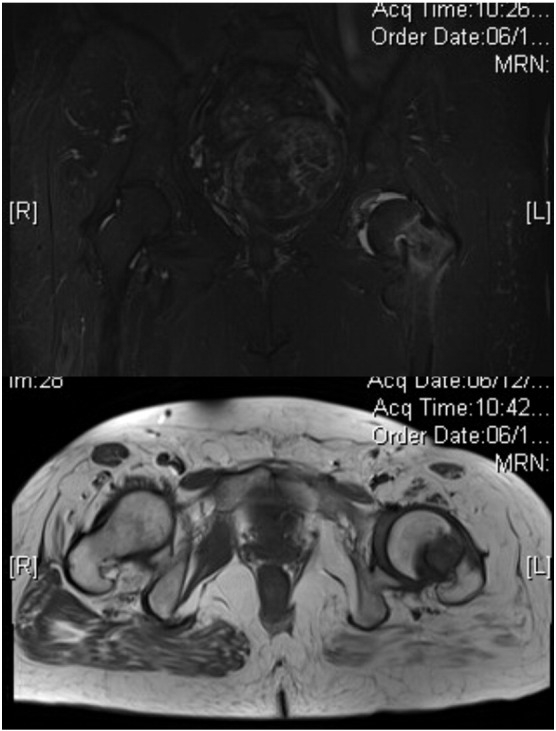
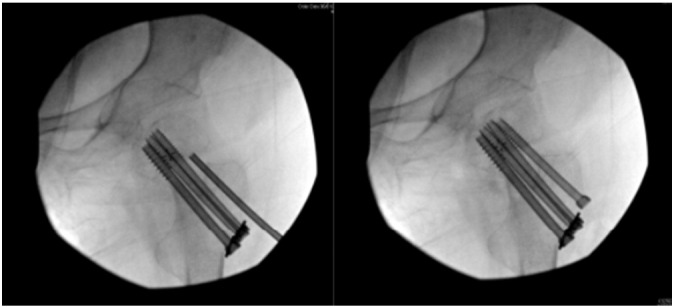
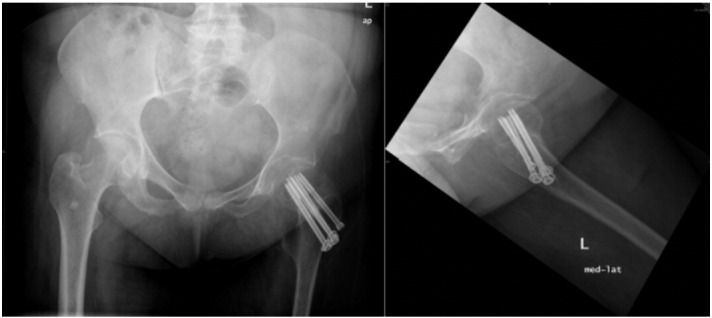
Poliomyelitis disease affects the anterior horns cells of the spinal cord and certain motor nuclei of the brain stem. Paralysis type is flaccid and asymmetrical and result in muscular imbalance. Due to this, in case of having a hip muscles involvement, degenerative or posttraumatic, total hip arthroplasty is normally contraindicated because of the excessive risk of hip dislocation. In cases of subcapital femoral neck fractures the femoral head vascularization is a main concern, and in cases of neglected fracture with pseudoarthrosis the vascular status to the head must be investigated prior to further decisions. We report the case of a femoral neck fracture non-union after a missed femoral neck fracture in a polio affected leg treated with cannulated screws and percutaneous autologous injection of processed total nuclear cells (TNC) mixed with putty demineralized bone matrix.
Keywords: Cell therapy; Femoral neck; Poliomyelitis; Pseudoarthrosis.
Figures


Similar articles
-
Total hip arthroplasty in paralytic dislocation from poliomyelitis.Orthopedics. 2008 Feb;31(2):179. doi: 10.3928/01477447-20080201-16. Orthopedics. 2008. PMID: 19292189
-
[Osteosynthesis of intracapsular femoral neck fractures by dynamic hip screw (DHS) fixation].Acta Chir Orthop Traumatol Cech. 2009 Aug;76(4):319-25. Acta Chir Orthop Traumatol Cech. 2009. PMID: 19755057 Czech.
-
[Surgical technique and early clinical outcomes of direct anterior approach to total hip arthroplasty].Beijing Da Xue Xue Bao Yi Xue Ban. 2017 Apr 18;49(2):206-213. Beijing Da Xue Xue Bao Yi Xue Ban. 2017. PMID: 28416826 Chinese.
-
Fractures of the femoral neck: a review and personal statement.Acta Chir Orthop Traumatol Cech. 2006;73(1):45-59. Acta Chir Orthop Traumatol Cech. 2006. PMID: 16613748 Review.
-
Subcapital femoral neck fracture after closed reduction and internal fixation of an intertrochanteric hip fracture: a case report and review of the literature.Am J Orthop (Belle Mead NJ). 1999 Sep;28(9):517-21. Am J Orthop (Belle Mead NJ). 1999. PMID: 10497859 Review.
Cited by
-
Total hip replacement in patient with residual poliomyelitis with neglected femoral neck fracture.BMJ Case Rep. 2021 May 21;14(5):e240221. doi: 10.1136/bcr-2020-240221. BMJ Case Rep. 2021. PMID: 34020986 Free PMC article.
References
-
- Aleem I.S., Karanicolas P.J., Bhandari M. Arthroplasty versus internal fixation of femoral neck fractures: a clinical decision analysis. Ortop. Traumatol. Rehabil. 2009;11:233. - PubMed
-
- Keating J.F., Grant A., Masson M., Scott N.W., Forbes J.F. Randomized comparison of reduction and fixation, bipolar hemiarthroplasty, and total hip arthroplasty: treatment of displaced intracapsular hip fractures in healthy older patients. J. Bone Joint Surg. Am. 2006;88-A:249–260. - PubMed
-
- Mathews V., Cabanela M.E. Femoral neck nonunion treatment. Clin. Orthop. Relat. Res. 2004;419:57–64. - PubMed
-
- Tidermark J. Quality of life and femoral neck fractures. Acta Orthop. Scand. Suppl. 2003;74:1–42. - PubMed
-
- Cameron H.U. Total hip replacement in a limb severely affected by paralytic poliomyelitis. Can. J. Surg. 1995;38:386. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
