

Imaging of urgencies and emergencies in the lung cancer patient
- PMID: 29644546
- PMCID: PMC6108967
- DOI: 10.1007/s13244-018-0605-6
Imaging of urgencies and emergencies in the lung cancer patient
Abstract
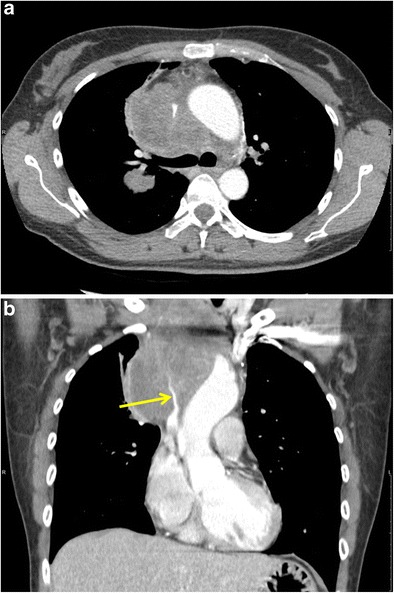
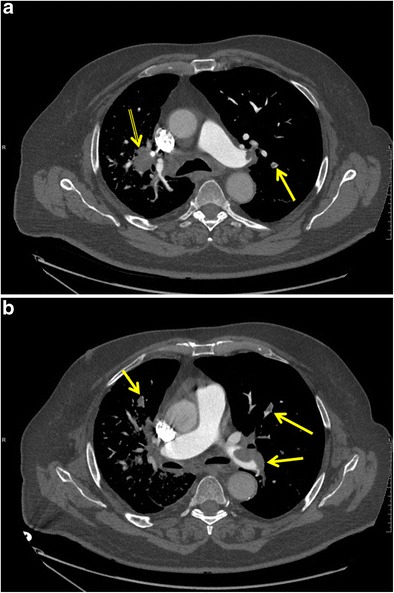
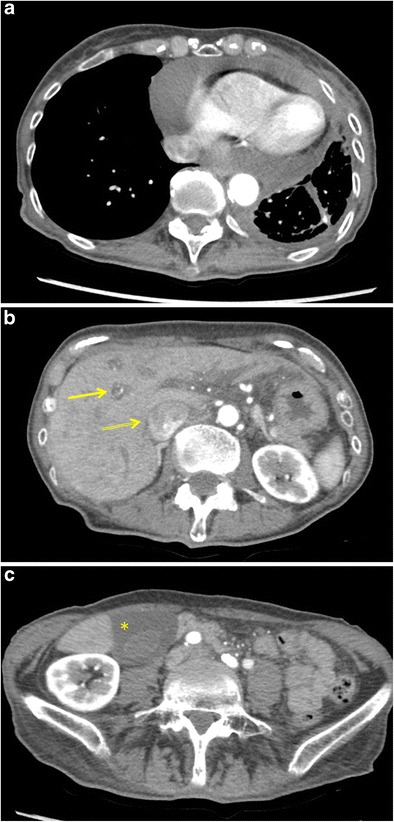
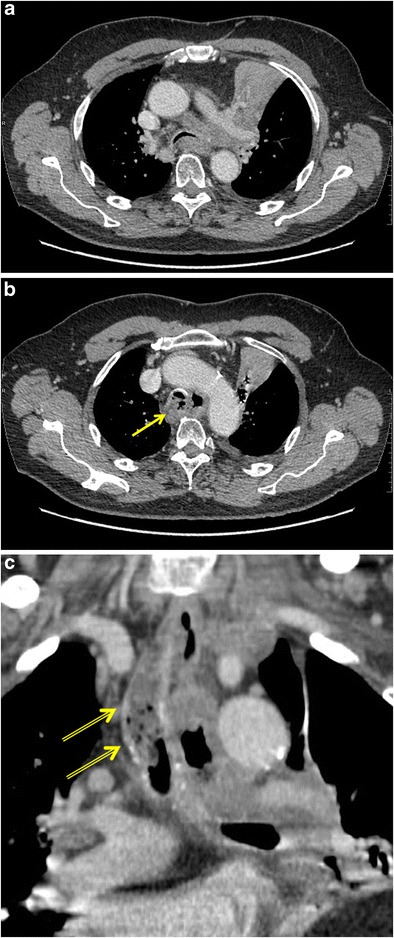
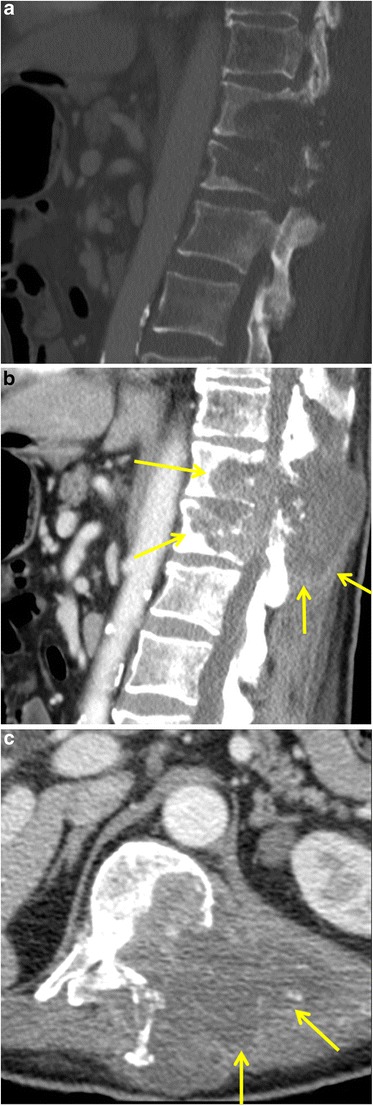
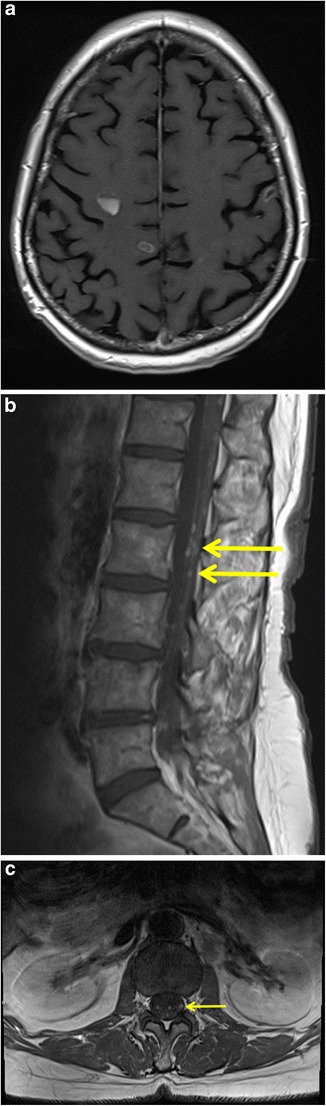
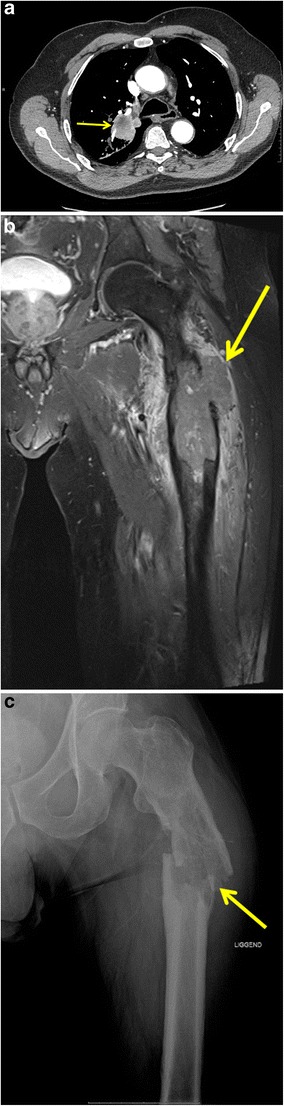
Lung cancer patients often experience potentially life-threatening medical urgencies and emergencies, which may be a direct or indirect result of the underlying malignancy. This pictorial review addresses the most common thoracic, neurological and musculoskeletal medical emergencies in lung cancer patients, including superior vena cava syndrome, pulmonary embolism, spontaneous pneumothorax, cardiac tamponade, massive haemoptysis, central airway obstruction, oesophagorespiratory fistula, malignant spinal cord compression, carcinomatous meningitis, cerebral herniation and pathological fracture. Emphasis is placed on imaging findings, the role of different imaging techniques and a brief discussion of epidemiology, pathophysiology and therapeutic options. Since early diagnosis is important for adequate patient management and prognosis, radiologists have a crucial role in recognising and communicating these urgencies and emergencies.
Teaching points: • Multiplanar multidetector computed tomography is the imaging examination of choice for thoracic urgencies and emergencies. • Magnetic resonance imaging is the imaging modality of choice for investigating central nervous system emergencies. • Urgencies and emergencies can be the initial manifestation of lung cancer. • Radiologists have a crucial role in recognising and in communicating these urgencies/emergencies.
Keywords: Computed tomography; Emergencies; Lung cancer; Magnetic resonance imaging; Radiography.
Conflict of interest statement
Conflicts of interest
All the authors declare that they have no conflict of interest.
Ethical adherence
The material in the manuscript has been acquired according to modern ethical standards.
Figures






References
-
- Lewis MA, Mayo C, Hendrickson AW, Mayo C, Moynihan TJ, Mayo C. Oncologic emergencies: Pathophysiology, presentation, diagnosis, and treatment. CA Cancer J Clin. 2011;61:287–314. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
