

Finger and forehead photoplethysmography-derived pulse-pressure variation and the benefits of baseline correction
- PMID: 29644558
- PMCID: PMC6314999
- DOI: 10.1007/s10877-018-0140-5
Finger and forehead photoplethysmography-derived pulse-pressure variation and the benefits of baseline correction
Abstract
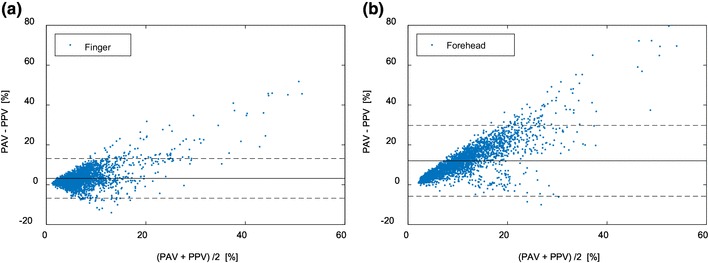
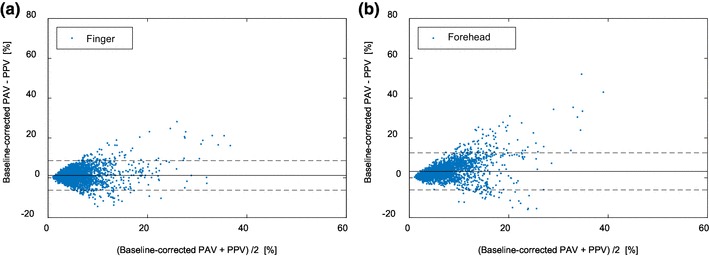
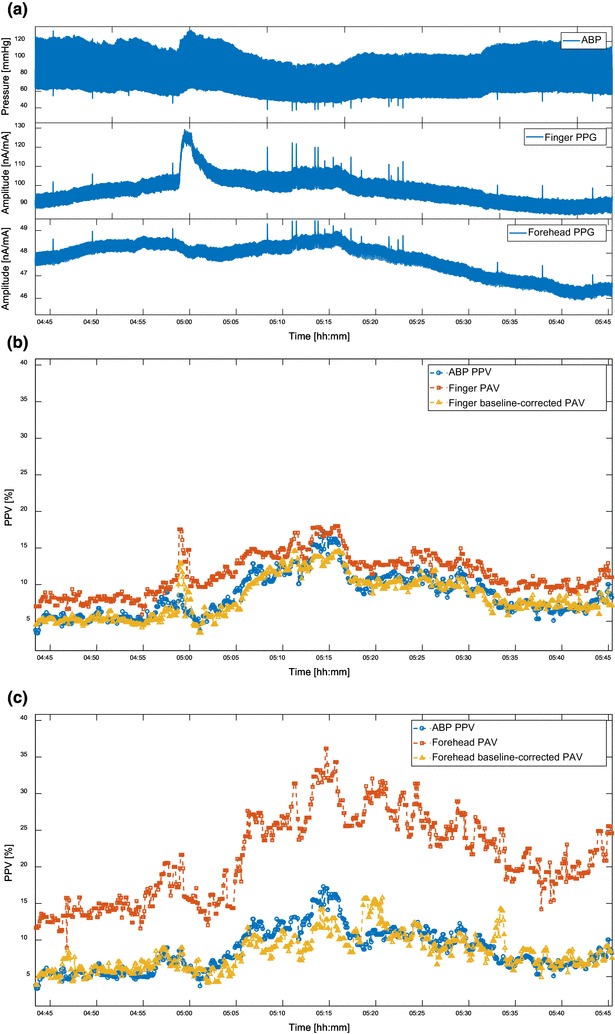
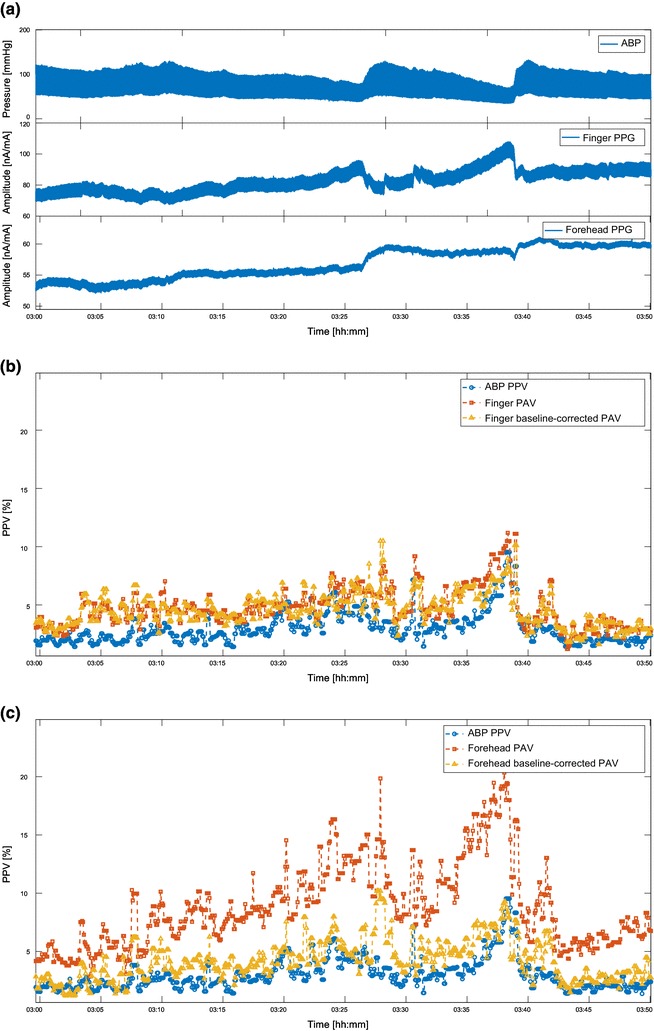
To non-invasively predict fluid responsiveness, respiration-induced pulse amplitude variation (PAV) in the photoplethysmographic (PPG) signal has been proposed as an alternative to pulse pressure variation (PPV) in the arterial blood pressure (ABP) signal. However, it is still unclear how the performance of the PPG-derived PAV is site-dependent during surgery. The aim of this study is to compare finger- and forehead-PPG derived PAV in their ability to approach the value and trend of ABP-derived PPV. Furthermore, this study investigates four potential confounding factors, (1) baseline variation, (2) PPV, (3) ratio of respiration and heart rate, and (4) perfusion index, which might affect the agreement between PPV and PAV. In this work, ABP, finger PPG, and forehead PPG were continuously recorded in 29 patients undergoing major surgery in the operating room. A total of 91.2 h data were used for analysis, from which PAV and PPV were calculated and compared. We analyzed the impact of the four factors using a multiple linear regression (MLR) analysis. The results show that compared with the ABP-derived PPV, finger-derived PAV had an agreement of 3.2 ± 5.1%, whereas forehead-PAV had an agreement of 12.0 ± 9.1%. From the MLR analysis, we found that baseline variation was a factor significantly affecting the agreement between PPV and PAV. After correcting for respiration-induced baseline variation, the agreements for finger- and forehead-derived PAV were improved to reach an agreement of - 1.2 ± 3.8% and 3.3 ± 4.8%, respectively. To conclude, finger-derived PAV showed better agreement with ABP-derived PPV compared to forehead-derived PAV. Baseline variation was a factor that significantly affected the agreement between PPV and PAV. By correcting for the baseline variation, improved agreements were obtained for both the finger and forehead, and the difference between these two agreements was diminished. The tracking abilities for both finger- and forehead-derived PAV still warrant improvement for wide use in clinical practice. Overall, our results show that baseline-corrected finger- and forehead-derived PAV may provide a non-invasive alternative for PPV.
Keywords: Fluid responsiveness; Major surgery; Photoplethysmography; Pulse pressure variation; Site dependency; Volume status.
Conflict of interest statement
Conflict of interest
Wouter H. Peeters, Rick Bezemer, Xi Long, Igor Paulussen, and Ronald M. Aarts are employed by Philips. Gerrit J. Noordergraaf is a consultant to Philips. Shaoxiong Sun is financially supported by a grant from China Scholarship Council (CSC).
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures
References
-
- Venn R, Steele A, Richardson P, Poloniecki J, Grounds M, Newman P. Randomized controlled trial to investigate influence of the fluid challenge on duration of hospital stay and perioperative morbidity in patients with hip fractures. Br J Anaesth. 2002;88(1):65–71. doi: 10.1093/bja/88.1.65. - DOI - PubMed
-
- Kumar A, Anel R, Bunnell E, et al. Pulmonary artery occlusion pressure and central venous pressure fail to predict ventricular filling volume, cardiac performance, or the response to volume infusion in normal subjects. Crit Care Med. 2004;32(3):691–699. doi: 10.1097/01.CCM.0000114996.68110.C9. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
