

Prognostic Evaluation of Neurological Assessment of the Neuro-Oncology Scale in Glioblastoma Patients
- PMID: 29644808
- PMCID: PMC5932296
- DOI: 10.14791/btrt.2018.6.e1
Prognostic Evaluation of Neurological Assessment of the Neuro-Oncology Scale in Glioblastoma Patients
Abstract
Background: The aims of this study were to investigate the role of the Neurological Assessment of Neuro-Oncology (NANO) scale in predicting the prognosis of patients with glioblastoma, and compare these results to predicted data of the Karnofsky Performance Scale (KPS), and Eastern Cooperative Oncology Group (ECOG)/World Health Organization (WHO) performance status. Additionally, we examined other prognostic factors in glioblastoma patients.
Methods: The medical records of 76 patients with a new diagnosis of histologically ascertained glioblastoma in the period from January 2002 to December 2015 at the authors' institution were retrospectively reviewed. Clinical factors, including epidemiologic, radiologic, and therapeutic values were reviewed as well as the performance status assessed by the KPS, ECOG/WHO performance status, and NANO scale.
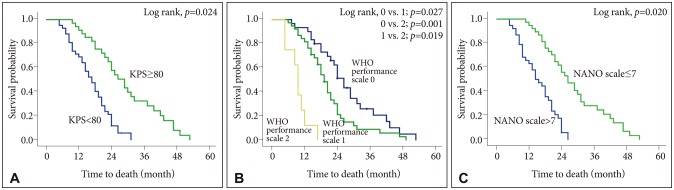
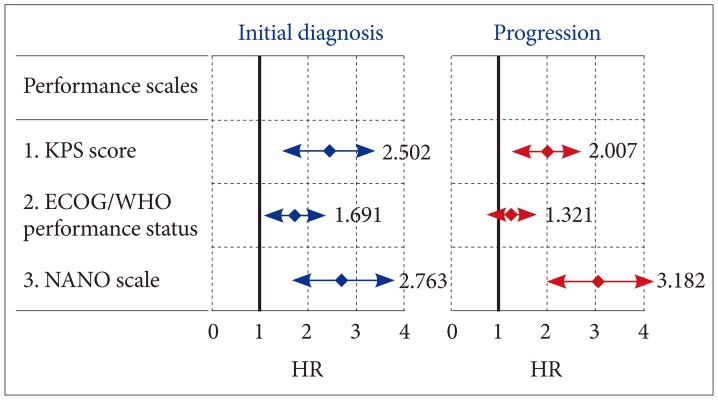
Results: The mean overall survival was 19.8 months (95% confidence interval 15.2-25.4 months). At initial diagnosis, the mean value [±standard deviation (SD)] of KPS score, ECOG/WHO performance status, and NANO scale were 81 (±7.4), 1.3 (±0.6), and 7.3 (±3.8), respectively. Multivariate analysis for predicting survival showed odds ratios of KPS score, ECOG/WHO performance status, and NANO scale were 2.502 (≥80 vs. <80; p=0.024), 1.691 (0-1 vs. 2-5; p=0.047), and 2.763 (0-7 vs. 8-23; p=0.020), respectively. At the time of progression, the mean value (±SD) of KPS score, ECOG/WHO performance status, and NANO scale were 69 (±8.2), 1.6 (±0.7), and 11.4 (±4.2), respectively; multivariate analysis for predicting survival showed that the odd ratios for KPS score, ECOG/WHO performance status, and NANO scale were 2.007 (≥80 vs. <80; p=0.035), 1.321 (0-1 vs. 2-5; p=0.143), and 3.182 (0-7 vs. 8-23; p=0.002), respectively.
Conclusion: The NANO scale provided a more detailed and objective measure of neurologic function than that currently used for predicting the prognosis of glioblastoma patients, especially at the time of progression.
Keywords: Glioblastoma; KPS; NANO scale; Prediction; Prognosis; Survival.
Copyright © 2018 The Korean Brain Tumor Society, The Korean Society for Neuro-Oncology, and The Korean Society for Pediatric Neuro-Oncology.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
Similar articles
-
Karnofsky Performance Scale and Neurological Assessment of Neuro-Oncology Scale as Early Predictor in Glioma.Asian Pac J Cancer Prev. 2020 Nov 1;21(11):3387-3392. doi: 10.31557/APJCP.2020.21.11.3387. Asian Pac J Cancer Prev. 2020. PMID: 33247700 Free PMC article.
-
The Neurologic Assessment in Neuro-Oncology (NANO) Scale as an Assessment Tool for Survival in Patients With Primary Glioblastoma.Neurosurgery. 2019 Mar 1;84(3):687-695. doi: 10.1093/neuros/nyy098. Neurosurgery. 2019. PMID: 29618103
-
Conversion of Karnofsky Performance Status (KPS) and Eastern Cooperative Oncology Group Performance Status (ECOG) to Palliative Performance Scale (PPS), and the interchangeability of PPS and KPS in prognostic tools.J Palliat Care. 2013 Autumn;29(3):163-9. J Palliat Care. 2013. PMID: 24380215
-
Inter-rater reliability in performance status assessment among healthcare professionals: an updated systematic review and meta-analysis.Support Care Cancer. 2020 May;28(5):2071-2078. doi: 10.1007/s00520-019-05261-7. Epub 2020 Jan 3. Support Care Cancer. 2020. PMID: 31900613
-
Prognostic value of ECOG performance status and Gleason score in the survival of castration-resistant prostate cancer: a systematic review.Asian J Androl. 2021 Mar-Apr;23(2):163-169. doi: 10.4103/aja.aja_53_20. Asian J Androl. 2021. PMID: 33159024 Free PMC article.
Cited by
-
Treatment, healthcare utilization and outcomes in patients with glioblastoma in Ontario: a 10-year cohort study.J Neurooncol. 2024 Jul;168(3):473-485. doi: 10.1007/s11060-024-04690-7. Epub 2024 May 3. J Neurooncol. 2024. PMID: 38702569
-
FACTORS AFFECTING OUTCOME IN THE TREATMENT OF GLIOBLASTOMA.Acta Clin Croat. 2022 Feb;60(3):373-378. doi: 10.20471/acc.2021.60.03.06. Acta Clin Croat. 2022. PMID: 35282478 Free PMC article.
-
Karnofsky Performance Scale and Neurological Assessment of Neuro-Oncology Scale as Early Predictor in Glioma.Asian Pac J Cancer Prev. 2020 Nov 1;21(11):3387-3392. doi: 10.31557/APJCP.2020.21.11.3387. Asian Pac J Cancer Prev. 2020. PMID: 33247700 Free PMC article.
-
Expression of some circulating microRNAs as predictive biomarkers for prognosis and treatment response in glioblastoma.Sci Rep. 2025 Jan 14;15(1):1933. doi: 10.1038/s41598-024-83800-x. Sci Rep. 2025. PMID: 39809835 Free PMC article.
-
Accelerated hyperfractionated radiochemotherapy with temozolomide is equivalent to normofractionated radiochemotherapy in a retrospective analysis of patients with glioblastoma.Radiat Oncol. 2019 Dec 12;14(1):227. doi: 10.1186/s13014-019-1427-5. Radiat Oncol. 2019. PMID: 31831026 Free PMC article.
References
-
- Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Ellison DW, Figarella-Branger D. Glioblastoma, IDH-wild-types. In: Louise DN, Brate DJ, Ohgaki H, et al., editors. WHO Classification of Tumours of the Central Nervous System. Rev 4th ed. Lyon: IARC Press; 2016. pp. 28–45.
-
- Hegi ME, Diserens AC, Gorlia T, et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med. 2005;352:997–1003. - PubMed
-
- Stupp R, Hegi ME, Mason WP, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–466. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
