

Prognosis of cardiovascular and non-cardiovascular multimorbidity after acute coronary syndrome
- PMID: 29649323
- PMCID: PMC5896917
- DOI: 10.1371/journal.pone.0195174
Prognosis of cardiovascular and non-cardiovascular multimorbidity after acute coronary syndrome
Abstract
Objective: To examine the prognosis of patients with cardiovascular and non-cardiovascular multimorbidity after acute coronary syndrome compared to patients without prior multimorbidity.
Methods: This multicenter prospective cohort study in Switzerland included 5,635 patients hospitalized with acute coronary syndrome between 2009 and 2014, with a one-year follow-up period. We defined cardiovascular and non-cardiovascular multimorbidity as having at least two prior comorbidities before the index hospitalization. Multivariable adjusted Cox proportional models were built to assess the one-year risk of recurrent cardiovascular events, defined as cardiovascular mortality and non-fatal myocardial infarction or stroke. The final model was adjusted for age, gender, body mass index, tobacco consumption, education, and family history of cardiovascular disease, prescription of high-dose statinsat discharge and use of cardiac rehabilitation after discharge.
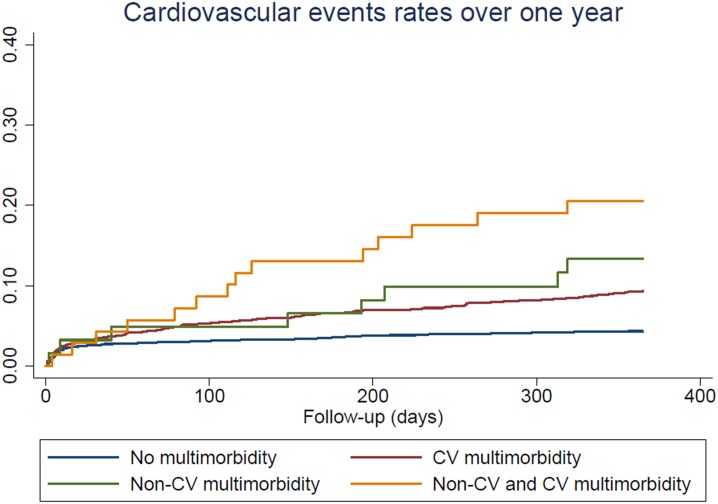
Results: Overall, 3,664 patients (65%) had no multimorbidity, 1,839 (33%) had cardiovascular multimorbidity, 62 (1%) had non-cardiovascular multimorbidity, and 70 (1%) had both cardiovascular and non-cardiovascular multimorbidity. The multivariate risk of recurrent cardiovascular events was increased among patients with cardiovascular multimorbidity (hazard ratio (HR) 2.05, 95% CI: 1.54-2.73, p<0.001) and patients with non-cardiovascular multimorbidity (HR 2.57, 95% CI: 1.04-6.35, p = 0.04) compared to patients without multimorbidity. Patients with cardiovascular and non-cardiovascular multimorbidity had the highest risk of recurrence with a HR of 5.19, 95% CI: 2.79-9.64, p<0.001, compared to patients without multimorbidity.
Conclusions: Multimorbidity increased by two-fold the risk of cardiovascular events over the year after an acute coronary syndrome. The magnitude of this increased risk was similar for patients with cardiovascular or non-cardiovascular multimorbidity.
Conflict of interest statement
Figures

References
-
- Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380(9836):37–43. Epub 2012/05/15. doi: 10.1016/S0140-6736(12)60240-2 . - DOI - PubMed
-
- Parekh AK, Barton MB. The challenge of multiple comorbidity for the us health care system. JAMA. 2010;303(13):1303–4. doi: 10.1001/jama.2010.381 - DOI - PubMed
-
- Farmer C, Fenu E, O'Flynn N, Guthrie B. Clinical assessment and management of multimorbidity: summary of NICE guidance. BMJ. 2016;354:i4843 Epub 2016/09/23. doi: 10.1136/bmj.i4843 . - DOI - PubMed
-
- Di Angelantonio E, Kaptoge S, Wormser D, Willeit P, Butterworth AS, Bansal N, et al. Association of Cardiometabolic Multimorbidity With Mortality. JAMA. 2015;314(1):52–60. doi: 10.1001/jama.2015.7008 . - DOI - PMC - PubMed
-
- Chen HY, Saczynski JS, McManus DD, Lessard D, Yarzebski J, Lapane KL, et al. The impact of cardiac and noncardiac comorbidities on the short-term outcomes of patients hospitalized with acute myocardial infarction: a population-based perspective. Clin Epidemiol. 2013;5:439–48. doi: 10.2147/CLEP.S49485 . - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
