

Image-guided radiotherapy reduces the risk of under-dosing high-risk prostate cancer extra-capsular disease and improves biochemical control
- PMID: 29650035
- PMCID: PMC5898030
- DOI: 10.1186/s13014-018-0978-1
Image-guided radiotherapy reduces the risk of under-dosing high-risk prostate cancer extra-capsular disease and improves biochemical control
Abstract
Background: To determine if reduced dose delivery uncertainty is associated with daily image-guidance (IG) and Prostate Specific Antigen Relapse Free Survival (PRFS) in intensity-modulated radiotherapy (IMRT) of high-risk prostate cancer (PCa).
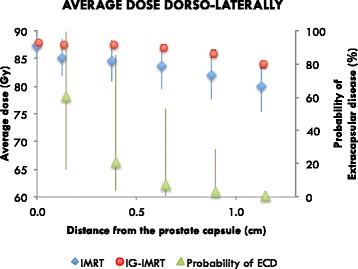
Methods: Planning data for consecutive PCa patients treated with IMRT (n = 67) and IG-IMRT (n = 35) was retrieved. Using computer simulations of setup errors, we estimated the patient-specific uncertainty in accumulated treatment dose distributions for the prostate and for posterolateral aspects of the gland that are at highest risk for extra-capsular disease. Multivariate Cox regression for PRFS considering Gleason score, T-stage, pre-treatment PSA, number of elevated clinical risk factors (T2c+, GS7+ and PSA10+), nomogram-predicted risk of extra-capsular disease (ECD), and dose metrics was performed.
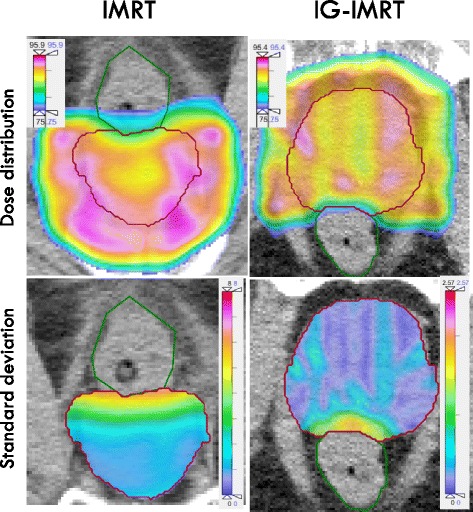
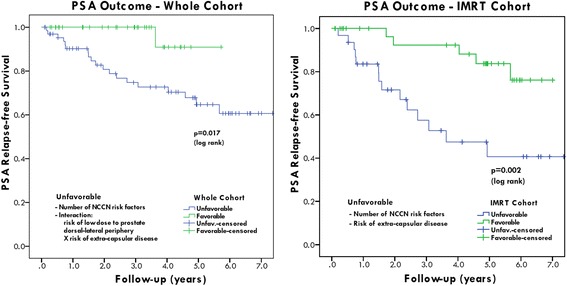
Results: For IMRT vs. IG-IMRT, plan dosimetry values were similar, but simulations revealed uncertainty in delivered dose external to the prostate was significantly different, due to positioning uncertainties. A patient-specific interaction term of the risk of ECD and risk of low dose to the ECD (p = 0.005), and the number of elevated clinical risk factors (p = 0.008), correlate with reduced PRFS.
Conclusions: Improvements in PSA outcomes for high-risk PCa using IG-IMRT vs. IMRT without IG may be due to improved dosimetry for ECD.
Keywords: High risk disease; IMRT; Image-guided; Prostate cancer; Radiotherapy; Tumor control probability.
Conflict of interest statement
Ethics approval and consent to participate
Data collection was approved by the local IRB.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Meijer GJ, de Klerk J, Bzdusek K, van den Berg HA, Janssen R, Kaus MR, et al. What CTV-to-PTV margins should be applied for prostate irradiation? Four-dimensional quantitative assessment using model-based deformable image registration techniques. Int J Radiat Oncol Biol Phys. 2008;72(5):1416–1425. doi: 10.1016/j.ijrobp.2008.03.005. - DOI - PubMed
-
- Vora SA, Wong WW, Schild SE, Ezzell GA, Halyard MY. Analysis of biochemical control and prognostic factors in patients treated with either low-dose three-dimensional conformal radiation therapy or high-dose intensity-modulated radiotherapy for localized prostate cancer. Int J Radiat Oncol Biol Phys. 2007;68(4):1053–1058. doi: 10.1016/j.ijrobp.2007.01.043. - DOI - PubMed
-
- Zelefsky MJ, Yamada Y, Fuks Z, Zhang Z, Hunt M, Cahlon O, et al. Long-term results of conformal radiotherapy for prostate cancer: impact of dose escalation on biochemical tumor control and distant metastases-free survival outcomes. Int J Radiat Oncol Biol Phys. 2008;71(4):1028–1033. doi: 10.1016/j.ijrobp.2007.11.066. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
