

Pro-Inflammatory Biomarkers in Stable Versus Acutely Decompensated Heart Failure With Preserved Ejection Fraction
- PMID: 29650706
- PMCID: PMC6015440
- DOI: 10.1161/JAHA.117.007385
Pro-Inflammatory Biomarkers in Stable Versus Acutely Decompensated Heart Failure With Preserved Ejection Fraction
Abstract
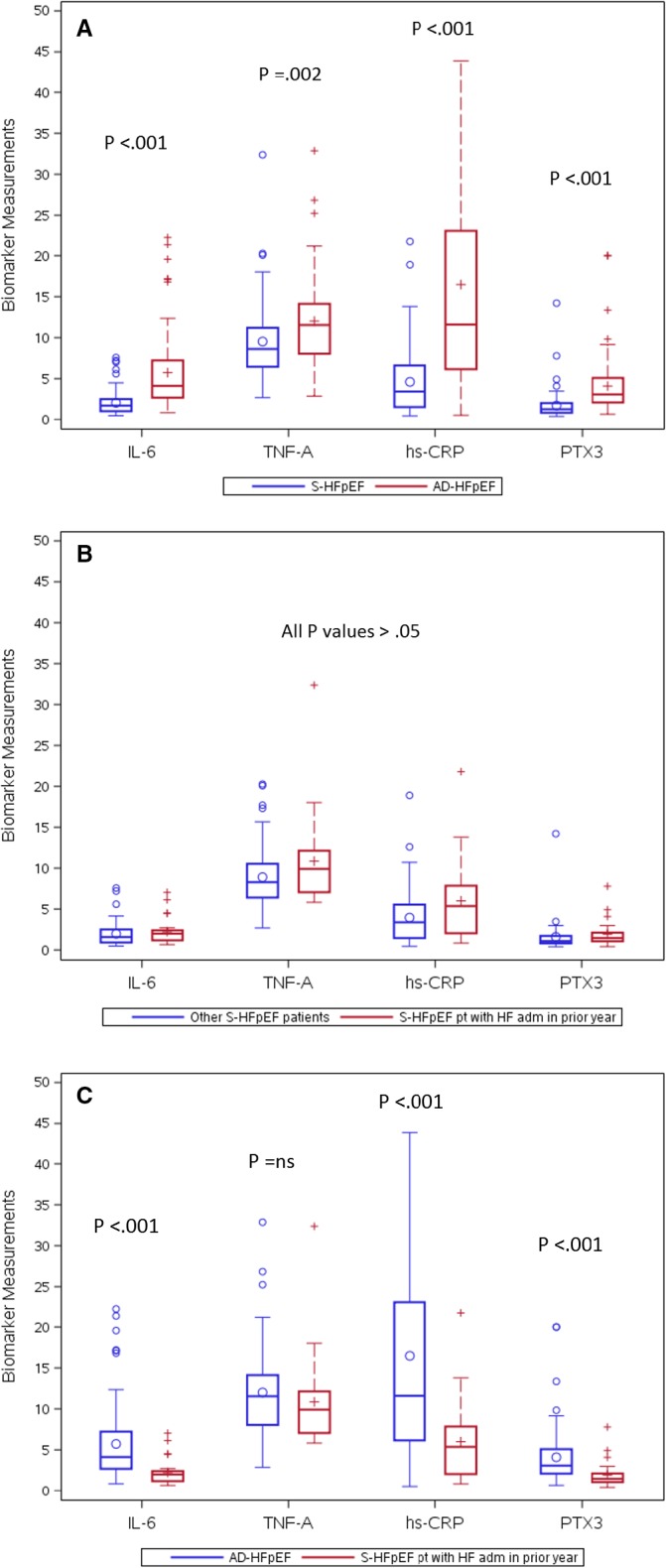
Background: Underlying inflammation has been increasingly recognized in heart failure with a preserved ejection fraction (HFpEF). In this study we tested the hypothesis that pro-inflammatory biomarkers are elevated in patients with acutely decompensated HFpEF (AD-HFpEF) compared with patients with stable HFpEF (S-HFpEF).
Methods and results: Using a post hoc analysis the serum biomarkers tumor necrosis factor-alpha, high-sensitivity C-reactive protein interleukin 6 and pentraxin 3 (PTX3) and clinical, demographic, echocardiographic-Doppler and clinical outcomes data were analyzed in HFpEF patients enrolled in NHLBI Heart Failure Research Network clinical trials which enrolled patients with either AD-HFpEF or S-HFpEF. Compared to S-HFpEF, AD-HFpEF patients had higher levels of PTX3 (3.08 ng/mL versus 1.27 ng/mL, P<0.0001), interleukin-6 (4.14 pg/mL versus 1.71 pg/mL, P<0.0001), tumor necrosis factor-alpha (11.54 pg/mL versus 8.62 pg/mL, P=0.0015), and high-sensitivity C-reactive protein (11.90 mg/dL versus 3.42 mg/dL, P<0.0001). Moreover, high-sensitivity C-reactive protein, interleukin-6 and PTX3 levels were significantly higher in AD-HFpEF compared with S-HFpEF patients admitted for decompensated HF within the previous year. PTX3 was positively correlated with left atrial volume index (r=0.41, P=0.0017) and left ventricular mass (r=0.26, P=0.0415), while tumor necrosis factor-alpha was inversely correlated with E/A ratio (r=-0.31, P=0.0395).
Conclusions: Levels of pro-inflammatory biomarkers are strikingly higher in AD-HFpEF compared with S-HFpEF patients. PTX3 and tumor necrosis factor-alpha are correlated with echocardiographic-Doppler evidence of diastolic dysfunction. Taken together these data support the concept that a heightened pro-inflammatory state has a pathophysiologic role in the development of AD-HFpEF.
Keywords: biomarker; decompensated heart failure; diastolic dysfunction; diastolic heart failure; ejection fraction; heart failure; pro‐inflammatory biomarkers.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Paulus WJ. Cytokines and heart failure. Heart Fail Monit. 2000;1:50–56. - PubMed
-
- D'Elia E, Vaduganathan M, Gori M, Gavazzi A, Butler J, Senni M. Role of biomarkers in cardiac structure phenotyping in heart failure with preserved ejection fraction: critical appraisal and practical use. Eur J Heart Fail. 2015;17:1231–1239. - PubMed
-
- Aukrust P, Ueland T, Muller F, Andreassen AK, Nordoy I, Aas H, Kjekshus J, Simonsen S, Freland SS, Gullestad L. Elevated circulating levels of C‐C chemokines in patients with congestive heart failure. Circulation. 1998;97:1136–1143. - PubMed
-
- Torre‐Amione G, Kapadia S, Benedict C, Oral H, Young JB, Mann DL. Proinflammatory cytokine levels in patients with depressed left ventricular ejection fraction: a report from the Studies of Left Ventricular Dysfunction (SOLVD). J Am Coll Cardiol. 1996;27:1201–1206. - PubMed
-
- Braunwald E. Biomarkers in heart failure. N Engl J Med. 2008;358:2148–2159. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 HL084904/HL/NHLBI NIH HHS/United States
- U01 HL084861/HL/NHLBI NIH HHS/United States
- U10 HL110312/HL/NHLBI NIH HHS/United States
- U01 HL084889/HL/NHLBI NIH HHS/United States
- U01 HL084890/HL/NHLBI NIH HHS/United States
- U01 HL084891/HL/NHLBI NIH HHS/United States
- U10 HL110342/HL/NHLBI NIH HHS/United States
- U10 HL110262/HL/NHLBI NIH HHS/United States
- U01 HL084931/HL/NHLBI NIH HHS/United States
- U10 HL110297/HL/NHLBI NIH HHS/United States
- U10 HL110302/HL/NHLBI NIH HHS/United States
- U10 HL110309/HL/NHLBI NIH HHS/United States
- U10 HL110336/HL/NHLBI NIH HHS/United States
- U10 HL110338/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
