

Cost-effectiveness of Continuous Glucose Monitoring for Adults With Type 1 Diabetes Compared With Self-Monitoring of Blood Glucose: The DIAMOND Randomized Trial
- PMID: 29650803
- PMCID: PMC5961392
- DOI: 10.2337/dc17-1821
Cost-effectiveness of Continuous Glucose Monitoring for Adults With Type 1 Diabetes Compared With Self-Monitoring of Blood Glucose: The DIAMOND Randomized Trial
Abstract
Objective: This study evaluated the societal cost-effectiveness of continuous glucose monitoring (CGM) in patients with type 1 diabetes (T1D) using multiple insulin injections.
Research design and methods: In the Multiple Daily Injections and Continuous Glucose Monitoring in Diabetes (DIAMOND) trial, 158 patients with T1D and HbA1c ≥7.5% were randomized in a 2:1 ratio to CGM or control. Participants were surveyed at baseline and 6 months. Within-trial and lifetime cost-effectiveness analyses were conducted. A modified Sheffield T1D policy model was used to simulate T1D complications. The main outcome was cost per quality-adjusted life-year (QALY) gained.
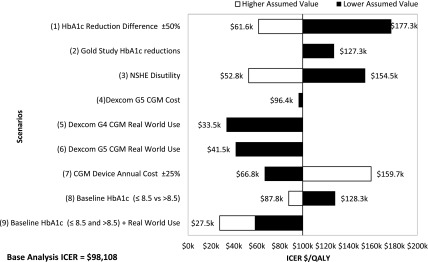
Results: Within the 6-month trial, the CGM group had similar QALYs to the control group (0.462 ± 0.05 vs. 0.455 ± 0.06 years, P = 0.61). The total 6-month costs were $11,032 (CGM) vs. $7,236 (control). The CGM group experienced reductions in HbA1c (0.60 ± 0.74% difference in difference [DiD]), P < 0.01), the daily rate of nonsevere hypoglycemia events (0.07 DiD, P = 0.013), and daily test strip use (0.55 ± 1.5 DiD, P = 0.04) compared with the control group. In the lifetime analysis, CGM was projected to reduce the risk of T1D complications and increase QALYs by 0.54. The incremental cost-effectiveness ratio (ICER) was $98,108 per QALY for the overall population. By extending sensor use from 7 to 10 days in a real-world scenario, the ICER was reduced to $33,459 per QALY.
Conclusions: For adults with T1D using multiple insulin injections and still experiencing suboptimal glycemic control, CGM is cost-effective at the willingness-to-pay threshold of $100,000 per QALY, with improved glucose control and reductions in nonsevere hypoglycemia.
© 2018 by the American Diabetes Association.
Figures
References
-
- American Diabetes Association Approaches to glycemic treatment. Sec 7. In Standards of Medical Care in Diabetes–2015. Diabetes Care 2015;38(Suppl. 1):S41–S48
-
- Miller KM, Foster NC, Beck RW, et al.; T1D Exchange Clinic Network . Current state of type 1 diabetes treatment in the U.S.: updated data from the T1D Exchange Clinic registry. Diabetes Care 2015;38:971–978 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
