

Exploring Variation in Glycemic Control Across and Within Eight High-Income Countries: A Cross-sectional Analysis of 64,666 Children and Adolescents With Type 1 Diabetes
- PMID: 29650804
- PMCID: PMC5961394
- DOI: 10.2337/dc17-2271
Exploring Variation in Glycemic Control Across and Within Eight High-Income Countries: A Cross-sectional Analysis of 64,666 Children and Adolescents With Type 1 Diabetes
Abstract
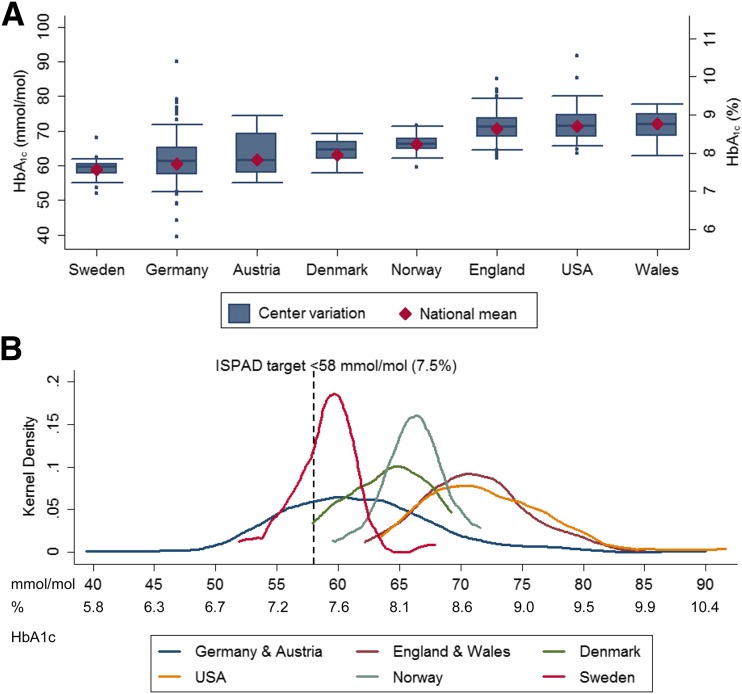
Objective: International studies on childhood type 1 diabetes (T1D) have focused on whole-country mean HbA1c levels, thereby concealing potential variations within countries. We aimed to explore the variations in HbA1c across and within eight high-income countries to best inform international benchmarking and policy recommendations.
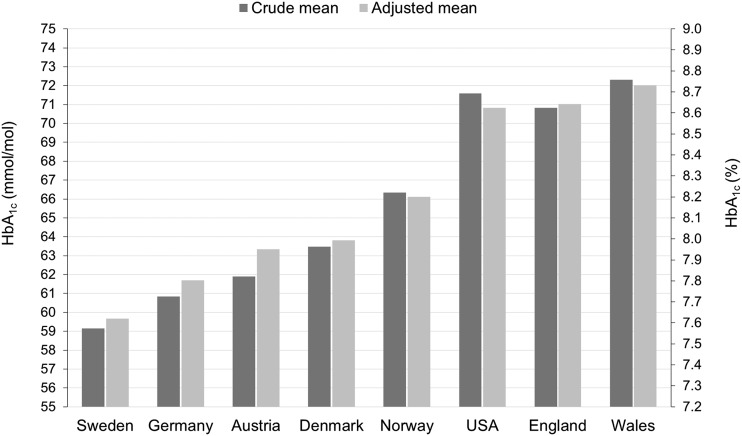
Research design and methods: Data were collected between 2013 and 2014 from 64,666 children with T1D who were <18 years of age across 528 centers in Germany, Austria, England, Wales, U.S., Sweden, Denmark, and Norway. We used fixed- and random-effects models adjusted for age, sex, diabetes duration, and minority status to describe differences between center means and to calculate the proportion of total variation in HbA1c levels that is attributable to between-center differences (intraclass correlation [ICC]). We also explored the association between within-center variation and children's glycemic control.
Results: Sweden had the lowest mean HbA1c (59 mmol/mol [7.6%]) and together with Norway and Denmark showed the lowest between-center variations (ICC ≤4%). Germany and Austria had the next lowest mean HbA1c (61-62 mmol/mol [7.7-7.8%]) but showed the largest center variations (ICC ∼15%). Centers in England, Wales, and the U.S. showed low-to-moderate variation around high mean values. In pooled analysis, differences between counties remained significant after adjustment for children characteristics and center effects (P value <0.001). Across all countries, children attending centers with more variable glycemic results had higher HbA1c levels (5.6 mmol/mol [0.5%] per 5 mmol/mol [0.5%] increase in center SD of HbA1c values of all children attending a specific center).
Conclusions: At similar average levels of HbA1c, countries display different levels of center variation. The distribution of glycemic achievement within countries should be considered in developing informed policies that drive quality improvement.
© 2018 by the American Diabetes Association.
Figures
References
-
- NICE Clinical Guideline. Diabetes (type 1 and type 2) in children and young people: diagnosis and management [article online], 2015. Available from https://www.nice.org.uk/guidance/ng18/resources/diabetes-type-1-and-type.... Accessed 15 February 2017
-
- Hofer S, Bauer M, Lanzersdorfer R, Walser I. Diabetes mellitus bei Kindern und Jugendlichen. Pädiatrie & Pädologie 2010;(Suppl. 3)
-
- Rewers MJ, Pillay K, de Beaufort C, et al.; International Society for Pediatric and Adolescent Diabetes . ISPAD Clinical Practice Consensus Guidelines 2014. Assessment and monitoring of glycemic control in children and adolescents with diabetes. Pediatr Diabetes 2014;15(Suppl. 20):102–114 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
