

Field validation of recombinant antigen immunoassays for diagnosis of Lassa fever
- PMID: 29651117
- PMCID: PMC5897328
- DOI: 10.1038/s41598-018-24246-w
Field validation of recombinant antigen immunoassays for diagnosis of Lassa fever
Abstract
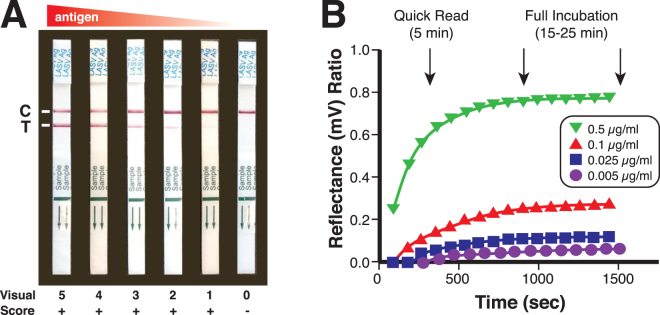
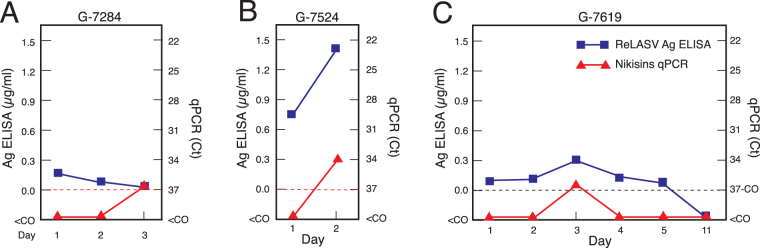
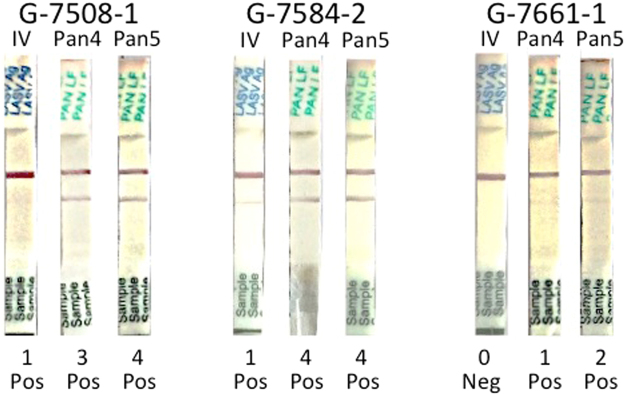
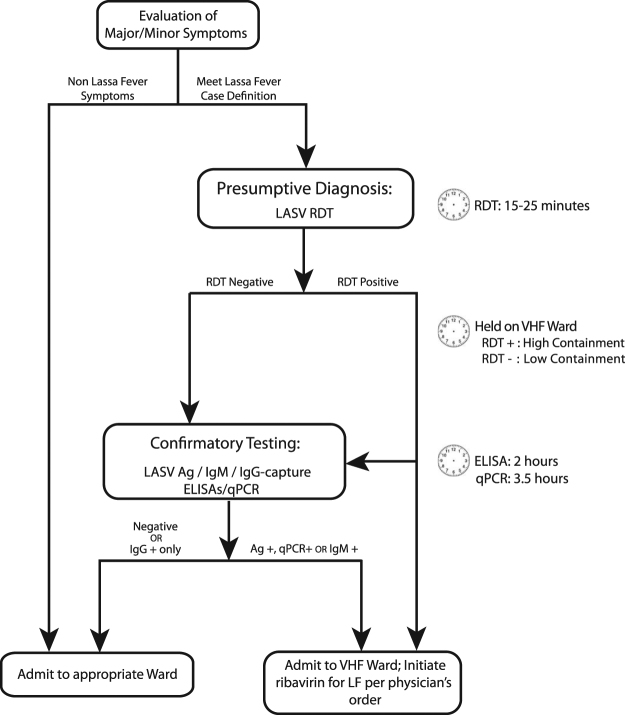
Lassa fever, a hemorrhagic fever caused by Lassa virus (LASV), is endemic in West Africa. It is difficult to distinguish febrile illnesses that are common in West Africa from Lassa fever based solely on a patient's clinical presentation. The field performance of recombinant antigen-based Lassa fever immunoassays was compared to that of quantitative polymerase chain assays (qPCRs) using samples from subjects meeting the case definition of Lassa fever presenting to Kenema Government Hospital in Sierra Leone. The recombinant Lassa virus (ReLASV) enzyme-linked immunosorbant assay (ELISA) for detection of viral antigen in blood performed with 95% sensitivity and 97% specificity using a diagnostic standard that combined results of the immunoassays and qPCR. The ReLASV rapid diagnostic test (RDT), a lateral flow immunoassay based on paired monoclonal antibodies to the Josiah strain of LASV (lineage IV), performed with 90% sensitivity and 100% specificity. ReLASV immunoassays performed better than the most robust qPCR currently available, which had 82% sensitivity and 95% specificity. The performance characteristics of recombinant antigen-based Lassa virus immunoassays indicate that they can aid in the diagnosis of LASV Infection and inform the clinical management of Lassa fever patients.
Conflict of interest statement
The Viral Hemorrhagic Fever Consortium (available at:
Figures



References
-
- WHO. Lassa Fever – Benin, Togo and Burkina Faso. Disease outbreak news 10 March 2017 (2017).
-
- ECDC. Lassa fever in Nigeria, Benin, Togo, Germany and USA. European Centre for Disease Prevention and Control 23 March 2016 (2016).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
